
Wednesday, May 5, 2010
"Healthy Families" Cuts
The recession has devastated Tout Tou Bounthapanya and her family. She's an immigrant who graduated from college. But she lost her job and depends on state sponsored health care. Bounthapanya said, "Because I use to be independent. I use to not be in any programs. I use to be independent ... If I apply for public programs, I'm not qualified like Medicare. If I apply for private market, it's too expensive. I can not afford them."
Bounthapanya is a recipient of "Healthy Families", a state program that provides affordable health care to working families. Governor Arnold Schwarzenegger wants to eliminate the program to help solve a $24-billion budget deficit.
Advocates like Reverend Sharon Stanley protested the cuts on Thursday in front of a West Fresno clinic. Stanely said, "We should not solve the budget crisis on the backs of the poorest we have in our county or any county around the state."
Doctors at Clinica Sierra Vista say "Healthy Families" actually saves money by providing preventative care and keeping people out of already crowded emergency rooms. Doctor Juan Carlos Ruvalcaba said, "It's a lot more expensive. I believe it's 10 times more expensive than coming to a primary care doctor ... They can wait up to 8-10 hours and take beds that real emergencies need to be taken care of."
Bounthapanya now wonders if her boys will lead healthy lives without the "Healthy families" program.
Taking the kids — and staying healthy
Sure the swine flu news is making us nervous — very nervous — just when millions of us are planning our much-needed summer vacations. But that doesn't mean we should grab the kids and huddle under the covers.
We just have to plan — and travel — smart. So far outbreaks have been reported in New York, California, Kansas, Ohio, Texas, Canada and even New Zealand with the first U.S. death reported Wednesday. The World Health Organization, which has upgraded the influenza alert level, says that given the widespread presence of the virus, current focus should be on "mitigation measures" and urges those who are ill to delay international travel and for those developing symptoms after an international trip to seek medical attention.
Of course, if we are smart, we're going to avoid "nonessential travel" to Mexico, as the Centers for Disease Control and Prevention has now recommended. (For the latest information, visit www.cdc.gov/travel.)
No worries if you have already booked a trip to Mexico. The airlines are waiving change fees and cruise lines are temporarily diverting ships. You should be able to either reschedule or get a refund without penalty for your hotel too. (And if you can't, let me know!)
With every resort offering incredible deals this summer, you shouldn't have trouble finding an alternate destination for some fun in the sun with the kids. (Check www.takingthekids.com for daily deals.)
At the same time, it's unclear if everyone is heeding the advice of health experts. Tim Smith, spokesman for American Airlines, says so far the airline is continuing to operate its normal schedule of 42 daily flights to Mexico. "No agency has asked us to reduce our schedule, though we obviously will continue to monitor demand." Smith notes that, so far, the volume of calls from customers seeking to change their Mexico itineraries has been far less than during a severe weather event.
The most important thing, of course, is to do all you can to keep the gang healthy wherever you're going. "Watch the news, since swine flu is an international problem affecting numerous countries," urges Dr. David Tayloe, the president of the American Academy of Pediatrics, who has traveled widely with his own four children.
Strict hand washing — at least a minute — is key, Dr. Tayloe adds.
"Bring hand sanitizer," adds Atlanta pediatrician and parenting author Dr. Jennifer Shu, editor of the American Academy of Pediatrics' book on baby and child health. "Teach kids not to touch their faces and avoid sick people!"
"The goal is to avoid crowds and close contact," says Dr. Meg Fisher, the chairman of the department of pediatrics at the Children's Hospital at Monmouth Medical Center and an infectious disease expert for the Academy of Pediatrics.
We just have to plan — and travel — smart. So far outbreaks have been reported in New York, California, Kansas, Ohio, Texas, Canada and even New Zealand with the first U.S. death reported Wednesday. The World Health Organization, which has upgraded the influenza alert level, says that given the widespread presence of the virus, current focus should be on "mitigation measures" and urges those who are ill to delay international travel and for those developing symptoms after an international trip to seek medical attention.
Of course, if we are smart, we're going to avoid "nonessential travel" to Mexico, as the Centers for Disease Control and Prevention has now recommended. (For the latest information, visit www.cdc.gov/travel.)
No worries if you have already booked a trip to Mexico. The airlines are waiving change fees and cruise lines are temporarily diverting ships. You should be able to either reschedule or get a refund without penalty for your hotel too. (And if you can't, let me know!)
With every resort offering incredible deals this summer, you shouldn't have trouble finding an alternate destination for some fun in the sun with the kids. (Check www.takingthekids.com for daily deals.)
At the same time, it's unclear if everyone is heeding the advice of health experts. Tim Smith, spokesman for American Airlines, says so far the airline is continuing to operate its normal schedule of 42 daily flights to Mexico. "No agency has asked us to reduce our schedule, though we obviously will continue to monitor demand." Smith notes that, so far, the volume of calls from customers seeking to change their Mexico itineraries has been far less than during a severe weather event.
The most important thing, of course, is to do all you can to keep the gang healthy wherever you're going. "Watch the news, since swine flu is an international problem affecting numerous countries," urges Dr. David Tayloe, the president of the American Academy of Pediatrics, who has traveled widely with his own four children.
Strict hand washing — at least a minute — is key, Dr. Tayloe adds.
"Bring hand sanitizer," adds Atlanta pediatrician and parenting author Dr. Jennifer Shu, editor of the American Academy of Pediatrics' book on baby and child health. "Teach kids not to touch their faces and avoid sick people!"
"The goal is to avoid crowds and close contact," says Dr. Meg Fisher, the chairman of the department of pediatrics at the Children's Hospital at Monmouth Medical Center and an infectious disease expert for the Academy of Pediatrics.
Saturday, April 17, 2010
White House Hosts Summit on Childhood Obesity

With one in three children falling into the overweight/obese category, this issue is approaching crisis mode. To stem the tide, and hopefully improve the health of our nation’s youth, the legislature, with the support of the White House, has been implementing programs, instituted the task force, and stumping for an improvement in our food delivery system overall and in our schools.
Back in February the White House announced the Healthy Food Financing Initiative, a $400 million/year initiative aimed to expand access to fresh, healthy food to all underserved urban and rural communities across the country within seven years, creating jobs in the process. During the same month, the First Lady launched her own childhood obesity initiative, “Let’s Move.” The program is quite ambitious, with the goal of developing workable ideas to help end childhood obesity within one generation.
The task force meeting, about 100 strong, was composed on senior Administration officials, doctors, teachers, activists, and other individuals who are committed to ending childhood obesity. Initial discussions focused on the cost of childhood obesity, the lack of playgrounds in neighborhoods around the country, and more esoteric issues such as behavioral economics. Melody Barnes, chairman of the task force and director of the Domestic Policy Council, broke the members into groups with a very specific task: "Come up with three to five of the best ideas, the important actions, the task force should recommend to the president."
It will be interesting to see what recommendations spring from this group of well-researched, knowledgeable individuals. Not only to they have to think outside the box, they need to think within a budget and at a level that works for children, parents, schools, and communities as a whole.
HealthNews Dozen: 12 Tips for Spring Allergies

But there are things one can do to minimize allergic reactions and the presence of allergens in many parts of one’s life. If the body’s immune system refuses to cooperate and fend off the allergy-causing substances, it is up to the person to change parts of their environment. Though it is humanly impossible to form a cocoon and hide there until summer, Prevention Magazine has some more realistic suggestions.
The first thing to do is engage in some spring cleaning. Wearing a mask while doing it may keep from being bombarded with dust during the process, but the cleaning is necessary. The artificial heat of winter and lack of fresh air often allows much dust to build in closets and in corners, and ridding the home of it all is the best way to start. However, it is necessary for allergy sufferers to continue to keep the home clean. Once the major scouring process is complete, a weekly surface-clean will keep the home a safe place for overly sensitive senses.
Spring cleaning might be the time to change things about one’s bed to make it an allergy-free zone as well. Special allergen-proof pillows are available at most home stores. And for those who have severe allergic reactions, there are mattresses and box springs that have tight fabric weaves to keep dust mites out.
Another change to the home is to add throw rugs. Even in a carpeted room, buying throw rugs can not only enhance the look of the room but allow the carpet to stay allergen free. And rugs can be easily cleaned in hot temperatures on a regular basis to kill dust mites.
Speaking of laundry, linens, towels, and the like should be washed in water that is at least 130 degrees, something that can be tested with a meat thermometer. If the home washer doesn’t reach a high enough temperature, a laundromat can wash to your specification.
Surrounding oneself with clean air is not always possible, but there are some things to do to make surroundings more allergy-free. In the car, use air conditioning rather than letting the wind blow allergens into the vehicle. Stay away from smoking and smokers, and if one must smoke, doing it outside to keep the home and vehicles free of smoke will help immensely. And in the house, a dehumidifier can stop many dust mite problems, as they don’t thrive in humidity below 45 percent. But if that doesn’t work, installing an air filter or air purifier can alleviate some of the problems.
A less ideal solution is to isolate pets in exchange for not getting rid of them altogether, but that is not realistic for most people who love their animals. There can be “safe” rooms, like the bedroom, however, where the pets are prohibited, which will allow some literal breathing room for those with allergies.
All in all, there are ways to ease the pain of allergy season. Though it may require more work than getting a prescription, it may be worth the better overall health of living in a cleaner environment and protecting oneself from mites and germs.
Privacy Policy
I respect your privacy and I am committed to safeguarding your privacy while online at my site publichealthfamily.blogspot.com. At .blogspot.com, the privacy of our visitors is of extreme importance to us. This privacy policy document outlines the types of personal information is received and collected by publichealthfamily.blogspot.com and how it is used.
Log Files
Like many other Web sites, publichealthfamily.blogspot.com makes use of log files. The information inside the log files includes internet protocol ( IP ) addresses, type of browser, Internet Service Provider ( ISP ), date/time stamp, referring/exit pages, and number of clicks to analyze trends, administer the site, track user’s movement around the site, and gather demographic information. IP addresses, and other such information are not linked to any information that is personally identifiable.
E-mail Subscription
If a user wishes to subscribe to my posts via e-mail (powered by Feedburner), I ask for contact information such as name and email address. Out of respect for my users’ privacy, a way to opt-out of these communications is provided.
Cookies and Web Beacons
A cookie is a piece of data stored on the user’s computer tied to information about the user. My site use cookies for tracking visitors’ activity. Some of our advertising partners may use cookies and web beacons on our site. Our advertising partners include Google Adsense. Please check their websites for respective privacy policies.
These third-party ad servers or ad networks use technology to the advertisements and links that appear on publichealthfamily.blogspot.com send directly to your browsers. They automatically receive your IP address when this occurs. Other technologies ( such as cookies, JavaScript, or Web Beacons ) may also be used by the third-party ad networks to measure the effectiveness of their advertisements and / or to personalize the advertising content that you see.
I use outside ad companies to display ads on my site. These ads may contain cookies and are collected by the ad companies, and I do not have no access to or control over these cookies that are used by third-party advertisers.
You should consult the respective privacy policies of these third-party ad servers for more detailed information on their practices as well as for instructions about how to opt-out of certain practices. publichealthfamily.blogspot.com's privacy policy does not apply to, and we cannot control the activities of, such other advertisers or web sites.
If you wish to disable cookies, you may do so through your individual browser options. More detailed information about cookie management with specific web browsers can be found at the browsers' respective websites.
Links
This Web site contains links to other sites. Please be aware that I am not responsible for the privacy practices of such other sites. I encourage my users to be aware when they leave our site and to read the privacy statements of each and every Web site that collects personally identifiable information. This privacy statement applies solely to information collected by this Web site.
Contact Information
If you require any more information or have any questions about our privacy policy, please feel free to contact us by email at tahshinaone@gmail.com.
Last Update
This Privacy Policy was last updated on September 7, 2009.
Log Files
Like many other Web sites, publichealthfamily.blogspot.com makes use of log files. The information inside the log files includes internet protocol ( IP ) addresses, type of browser, Internet Service Provider ( ISP ), date/time stamp, referring/exit pages, and number of clicks to analyze trends, administer the site, track user’s movement around the site, and gather demographic information. IP addresses, and other such information are not linked to any information that is personally identifiable.
E-mail Subscription
If a user wishes to subscribe to my posts via e-mail (powered by Feedburner), I ask for contact information such as name and email address. Out of respect for my users’ privacy, a way to opt-out of these communications is provided.
Cookies and Web Beacons
A cookie is a piece of data stored on the user’s computer tied to information about the user. My site use cookies for tracking visitors’ activity. Some of our advertising partners may use cookies and web beacons on our site. Our advertising partners include Google Adsense. Please check their websites for respective privacy policies.
These third-party ad servers or ad networks use technology to the advertisements and links that appear on publichealthfamily.blogspot.com send directly to your browsers. They automatically receive your IP address when this occurs. Other technologies ( such as cookies, JavaScript, or Web Beacons ) may also be used by the third-party ad networks to measure the effectiveness of their advertisements and / or to personalize the advertising content that you see.
I use outside ad companies to display ads on my site. These ads may contain cookies and are collected by the ad companies, and I do not have no access to or control over these cookies that are used by third-party advertisers.
You should consult the respective privacy policies of these third-party ad servers for more detailed information on their practices as well as for instructions about how to opt-out of certain practices. publichealthfamily.blogspot.com's privacy policy does not apply to, and we cannot control the activities of, such other advertisers or web sites.
If you wish to disable cookies, you may do so through your individual browser options. More detailed information about cookie management with specific web browsers can be found at the browsers' respective websites.
Links
This Web site contains links to other sites. Please be aware that I am not responsible for the privacy practices of such other sites. I encourage my users to be aware when they leave our site and to read the privacy statements of each and every Web site that collects personally identifiable information. This privacy statement applies solely to information collected by this Web site.
Contact Information
If you require any more information or have any questions about our privacy policy, please feel free to contact us by email at tahshinaone@gmail.com.
Last Update
This Privacy Policy was last updated on September 7, 2009.
Thursday, April 15, 2010
Copper in Food
Sources of Copper
It isn't hard to get enough copper-- unless you live in an industrial nation. I've compiled a chart showing the copper content of various refined and unrefined foods to illustrate the point. The left side shows industrial staple foods, while the right side shows whole foods. I've incorporated a few that would have been typical of Polynesian and Melanesian cultures apparently free of cardiovascular disease. The serving sizes are what one might reasonably eat at a meal: roughly 200 calories for grains, tubers and whole coconut; 1/4 pound for animal products; 1/2 teaspoon for salt; 1 cup for raw kale; 1 oz for sugar.
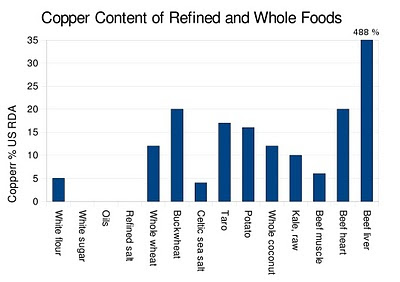 Note that beef liver is off the chart at 488 percent of the USDA recommended daily allowance. I don't know if you'd want to sit down and eat a quarter pound of beef liver, but you get the picture. Beef liver is nature's multivitamin: hands down the Most Nutritious Food in the World. That's because it acts as a storage depot for a number of important micronutrients, as well as being a biochemical factory that requires a large amount of B vitamins to function. You can see that muscle tissue isn't a great source of copper compared to other organs, and this holds true for other micronutrients as well.
Note that beef liver is off the chart at 488 percent of the USDA recommended daily allowance. I don't know if you'd want to sit down and eat a quarter pound of beef liver, but you get the picture. Beef liver is nature's multivitamin: hands down the Most Nutritious Food in the World. That's because it acts as a storage depot for a number of important micronutrients, as well as being a biochemical factory that requires a large amount of B vitamins to function. You can see that muscle tissue isn't a great source of copper compared to other organs, and this holds true for other micronutrients as well.
Beef liver is so full of micronutrients, it shouldn't be eaten every day. Think of it in terms of the composition of a cow's body. The edible carcass is mostly muscle, but a significant portion is liver. I think it makes sense to eat some form of liver about once per week.
Modern Agriculture Produces Micronutrient-poor Foods
The numbers in the graph above come from NutritionData, my main source of food nutrient composition. The problem with relying on this kind of information is it ignores the variability in micronutrient content due to plant strain, soil quality, et cetera.
The unfortunate fact is that micronutrient levels have declined substantially over the course of the 20th century, even in whole foods. Dr. Donald R. Davis has documented the substantial decline in copper and other micronutrients in American foods over the second half of the last century (1). An even more marked decrease has occurred in the UK (2), with similar trends worldwide. On average, the copper content of vegetables in the UK has declined 76 percent since 1940. Most of the decrease has taken place since 1978. Fruits are down 20 percent and meats are down 24 percent.
I find this extremely disturbing, as it will affect even people eating whole food diets. This is yet another reason to buy from artisanal producers, who are likely to use more traditional plant varieties and grow in richer soil. Grass-fed beef should be just as nutritious as it has always been. Some people may also wish to grow, hunt or fish their own food.
It isn't hard to get enough copper-- unless you live in an industrial nation. I've compiled a chart showing the copper content of various refined and unrefined foods to illustrate the point. The left side shows industrial staple foods, while the right side shows whole foods. I've incorporated a few that would have been typical of Polynesian and Melanesian cultures apparently free of cardiovascular disease. The serving sizes are what one might reasonably eat at a meal: roughly 200 calories for grains, tubers and whole coconut; 1/4 pound for animal products; 1/2 teaspoon for salt; 1 cup for raw kale; 1 oz for sugar.
 Note that beef liver is off the chart at 488 percent of the USDA recommended daily allowance. I don't know if you'd want to sit down and eat a quarter pound of beef liver, but you get the picture. Beef liver is nature's multivitamin: hands down the Most Nutritious Food in the World. That's because it acts as a storage depot for a number of important micronutrients, as well as being a biochemical factory that requires a large amount of B vitamins to function. You can see that muscle tissue isn't a great source of copper compared to other organs, and this holds true for other micronutrients as well.
Note that beef liver is off the chart at 488 percent of the USDA recommended daily allowance. I don't know if you'd want to sit down and eat a quarter pound of beef liver, but you get the picture. Beef liver is nature's multivitamin: hands down the Most Nutritious Food in the World. That's because it acts as a storage depot for a number of important micronutrients, as well as being a biochemical factory that requires a large amount of B vitamins to function. You can see that muscle tissue isn't a great source of copper compared to other organs, and this holds true for other micronutrients as well.Beef liver is so full of micronutrients, it shouldn't be eaten every day. Think of it in terms of the composition of a cow's body. The edible carcass is mostly muscle, but a significant portion is liver. I think it makes sense to eat some form of liver about once per week.
Modern Agriculture Produces Micronutrient-poor Foods
The numbers in the graph above come from NutritionData, my main source of food nutrient composition. The problem with relying on this kind of information is it ignores the variability in micronutrient content due to plant strain, soil quality, et cetera.
The unfortunate fact is that micronutrient levels have declined substantially over the course of the 20th century, even in whole foods. Dr. Donald R. Davis has documented the substantial decline in copper and other micronutrients in American foods over the second half of the last century (1). An even more marked decrease has occurred in the UK (2), with similar trends worldwide. On average, the copper content of vegetables in the UK has declined 76 percent since 1940. Most of the decrease has taken place since 1978. Fruits are down 20 percent and meats are down 24 percent.
I find this extremely disturbing, as it will affect even people eating whole food diets. This is yet another reason to buy from artisanal producers, who are likely to use more traditional plant varieties and grow in richer soil. Grass-fed beef should be just as nutritious as it has always been. Some people may also wish to grow, hunt or fish their own food.
Tuesday, April 13, 2010
Interview with John Barban
I recently did a podcast interview with John Barban from the Adonis Lifestyle blog. We talked mostly about fat mass and the body fat "setpoint". As it turns out, what I said must have been at odds with John's philosophy, because he posted another podcast the next week that appears to be about why he disagrees with me!
Anyway, enjoy the interview.
I did another one recently with Jimmy Moore that's coming soon.
Anyway, enjoy the interview.
I did another one recently with Jimmy Moore that's coming soon.
Monday, April 12, 2010
Gary Taubes Speaks this Thursday at UW
Gary Taubes will be giving a lecture this Thursday, April 15th, at the University of Washington in Seattle, titled "Why we get fat: adiposity 101 and an alternative hypothesis of obesity". It's free and open to the public. The talk is from noon to 1:00, followed by a question and answer session from 1:00 to 2:00.
The talk will take place in Hogness auditorium, which is room A420 of the Health Sciences building (1959 NE Pacific St). The whole area is difficult to navigate, so allow yourself time to park and find the auditorium. Here are directions to Hogness, including parking.
I'll be sitting near the front if anyone wants to say hi afterward.
The talk will take place in Hogness auditorium, which is room A420 of the Health Sciences building (1959 NE Pacific St). The whole area is difficult to navigate, so allow yourself time to park and find the auditorium. Here are directions to Hogness, including parking.
I'll be sitting near the front if anyone wants to say hi afterward.
Friday, April 9, 2010
Full-fat Dairy for Cardiovascular Health
I just saw a paper in the AJCN titled "Dairy consumption and patterns of mortality of
Australian adults". It's a prospective study with a 15-year follow-up period. Here's a quote from the abstract:
Contrary to popular belief, full-fat dairy, including milk, butter and cheese, has never been convincingly linked to cardiovascular disease. In fact, it has rather consistently been linked to a lower risk, particularly for stroke. What has been linked to cardiovascular disease is milk fat's replacement, margarine. In the Rotterdam study, high vitamin K2 intake was linked to a lower risk of fatal heart attack, aortic calcification and all-cause mortality. Most of the K2 came from full-fat cheese. In my opinion, artisanal cheese and butter made from pasture-fed milk are the ultimate dairy foods.
From a 2005 literature review on milk and cardiovascular disease in the EJCN:
Australian adults". It's a prospective study with a 15-year follow-up period. Here's a quote from the abstract:
There was no consistent and significant association between total dairy intake and total or cause-specific mortality. However, compared with those with the lowest intake of full-fat dairy, participants with the highest intake (median intake 339 g/day) had reduced death due to CVD (HR: 0.31; 95% confidence interval (CI): 0.12–0.79; P for trend = 0.04) after adjustment for calcium intake and other confounders. Intakes of low-fat dairy, specific dairy foods, calcium and vitamin D showed no consistent associations.People who ate the most full-fat dairy had a 69% lower risk of cardiovascular death than those who ate the least. Otherwise stated, people who mostly avoided dairy or consumed low-fat dairy had more than three times the risk of dying of coronary heart disease or stroke than people who ate the most full-fat diary.
Contrary to popular belief, full-fat dairy, including milk, butter and cheese, has never been convincingly linked to cardiovascular disease. In fact, it has rather consistently been linked to a lower risk, particularly for stroke. What has been linked to cardiovascular disease is milk fat's replacement, margarine. In the Rotterdam study, high vitamin K2 intake was linked to a lower risk of fatal heart attack, aortic calcification and all-cause mortality. Most of the K2 came from full-fat cheese. In my opinion, artisanal cheese and butter made from pasture-fed milk are the ultimate dairy foods.
From a 2005 literature review on milk and cardiovascular disease in the EJCN:
In total, 10 studies were identified. Their results show a high degree of consistency in the reported risk for heart disease and stroke, all but one study suggesting a relative risk of less than one in subjects with the highest intakes of milk.The fat is where the vitamins A, K2, E and D are. The fat is where the medium-chain triglycerides, butyric acid and omega-3 fatty acids are. The fat is where the conjugated linoleic acid is. So the next time someone admonishes you to reduce your dairy fat intake, what are you going to tell them??
...the studies, taken together, suggest that milk drinking may be associated with a small but worthwhile reduction in heart disease and stroke risk.
...All the cohort studies in the present review had, however, been set up at times when reduced-fat milks were unavailable, or scarce.
Tuesday, April 6, 2010
Copper and Cardiovascular Disease
In 1942, Dr. H. W. Bennetts dissected 21 cattle known to have died of "falling disease". This was the name given to the sudden, inexplicable death that struck herds of cattle in certain regions of Australia. Dr. Bennett believed the disease was linked to copper deficiency. He found that 19 of the 21 cattle had abnormal hearts, showing atrophy and abnormal connective tissue infiltration (fibrosis) of the heart muscle (1).
In 1963, Dr. W. F. Coulson and colleagues found that 22 of 33 experimental copper-deficient pigs died of cardiovascular disease. 11 of 33 died of coronary heart disease, the quintessential modern human cardiovascular disease. Pigs on a severely copper-deficient diet showed weakened and ruptured arteries (aneurysms), while moderately deficient pigs "survived with scarred vessels but demonstrated a tendency toward premature atherosclerosis" including foam cell accumulation (2). Also in 1963, Dr. C. R. Ball and colleagues published a paper describing blood clots in the heart and coronary arteries, heart muscle degeneration, ventricular calcification and early death in mice fed a lard-rich diet (3).
This is where Dr. Leslie M. Klevay enters the story. Dr. Klevay suspected that Ball's mice had suffered from copper deficiency, and decided to test the hypothesis. He replicated Ball's experiment to the letter, using the same strain of mice and the same diet. Like Ball, he observed abnormal clotting in the heart, degeneration and enlargement of the heart muscle, and early death. He also showed by electrocardiogram that the hearts of the copper-deficient mice were often contracting abnormally (arrhythmia).
But then the coup de grace: he prevented these symptoms by supplementing the drinking water of a second group of mice with copper (4). In the words of Dr. Klevay: "copper was an antidote to fat intoxication" (5). I believe this was his tongue-in-cheek way of saying that the symptoms had been misdiagnosed by Ball as due to dietary fat, when in fact they were due to a lack of copper.
Since this time, a number of papers have been published on the relationship between copper intake and cardiovascular disease in animals, including several showing that copper supplementation prevents atherosclerosis in one of the most commonly used animal models of cardiovascular disease (6, 7, 8). Copper supplementation also corrects abnormal heart enlargement-- called hypertrophic cardiomyopathy-- and heart failure due to high blood pressure in mice (9).
For more than three decades, Dr. Klevay has been a champion of the copper deficiency theory of cardiovascular disease. According to him, copper deficiency is the only single intervention that has caused the full spectrum of human cardiovascular disease in animals, including:
The second reason you may not have heard of the theory is due to a lab assay called copper-mediated LDL oxidation. Researchers take LDL particles (from blood, the same ones the doctor measures as part of a cholesterol test) and expose them to a high concentration of copper in a test tube. Free copper ions are oxidants, and the researchers then measure the amount of time it takes the LDL to oxidize. I find this assay tiresome, because studies have shown that the amount of time it takes copper to oxidize LDL in a test tube doesn't predict how much oxidized LDL you'll actually find in the bloodstream of the person you took the LDL from (10, 11).
In other words, it's an assay that has little bearing on real life. But researchers like it because for some odd reason, feeding a person saturated fat causes their LDL to be oxidized more rapidly by copper in a test tube, even though that's not the case in the actual bloodstream (12). Guess which result got emphasized?
The fact that copper is such an efficient oxidant has led some researchers to propose that copper oxidizes LDL in human blood, and therefore dietary copper may contribute to heart disease (oxidized LDL is a central player in heart disease-- read more here). The problem with this theory is that there are virtually zero free copper ions in human serum. Then there's the fact that supplementing humans with copper actually reduces the susceptibility of red blood cells to oxidation (by copper in a test tube, unfortunately), which is difficult to reconcile with the idea that dietary copper increases oxidative stress in the blood (13).
The third reason you may never have heard of the theory is more problematic. Several studies have found that a higher level copper in the blood correlates with a higher risk of heart attack (14, 15). At this point, I could hang up my hat, and declare the animal experiments irrelevant to humans. But let's dig deeper.
Nutrient status is sometimes a slippery thing to measure. As it turns out, serum copper isn't a good marker of copper status. In a 4-month trial of copper depletion in humans, blood copper stayed stable, while the activity of copper-dependent enzymes in the blood declined (16). These include the important copper-dependent antioxidant, superoxide dismutase. As a side note, lysyl oxidase is another copper-dependent enzyme that cross-links the important structural proteins collagen and elastin in the artery wall, potentially explaining some of the vascular consequences of copper deficiency. Clotting factor VIII increased dramatically during copper depletion, perhaps predicting an increased tendency to clot. Even more troubling, three of the 12 women developed heart problems during the trial, which the authors felt was unusual:
Only a few studies have looked at the relationship between more accurate markers of copper status and cardiovascular disease in humans. Leukocyte copper status, a marker of tissue status, is lower in people with cardiovascular disease (22, 23). People who die of heart attacks generally have less copper in their hearts than people who die of other causes, although this could be an effect rather than a cause of the heart attack (24). Overall, I find the human data lacking. I'd like to see more studies examining liver copper status in relation to cardiovascular disease, as the liver is the main storage organ for copper.
According to a 2001 study, the majority of Americans may have copper intakes below the USDA recommended daily allowance (25), many substantially so. This problem is exacerbated by the fact that copper levels in food have declined in industrial nations over the course of the 20th century, something I'll discuss in the next post.
In 1963, Dr. W. F. Coulson and colleagues found that 22 of 33 experimental copper-deficient pigs died of cardiovascular disease. 11 of 33 died of coronary heart disease, the quintessential modern human cardiovascular disease. Pigs on a severely copper-deficient diet showed weakened and ruptured arteries (aneurysms), while moderately deficient pigs "survived with scarred vessels but demonstrated a tendency toward premature atherosclerosis" including foam cell accumulation (2). Also in 1963, Dr. C. R. Ball and colleagues published a paper describing blood clots in the heart and coronary arteries, heart muscle degeneration, ventricular calcification and early death in mice fed a lard-rich diet (3).
This is where Dr. Leslie M. Klevay enters the story. Dr. Klevay suspected that Ball's mice had suffered from copper deficiency, and decided to test the hypothesis. He replicated Ball's experiment to the letter, using the same strain of mice and the same diet. Like Ball, he observed abnormal clotting in the heart, degeneration and enlargement of the heart muscle, and early death. He also showed by electrocardiogram that the hearts of the copper-deficient mice were often contracting abnormally (arrhythmia).
But then the coup de grace: he prevented these symptoms by supplementing the drinking water of a second group of mice with copper (4). In the words of Dr. Klevay: "copper was an antidote to fat intoxication" (5). I believe this was his tongue-in-cheek way of saying that the symptoms had been misdiagnosed by Ball as due to dietary fat, when in fact they were due to a lack of copper.
Since this time, a number of papers have been published on the relationship between copper intake and cardiovascular disease in animals, including several showing that copper supplementation prevents atherosclerosis in one of the most commonly used animal models of cardiovascular disease (6, 7, 8). Copper supplementation also corrects abnormal heart enlargement-- called hypertrophic cardiomyopathy-- and heart failure due to high blood pressure in mice (9).
For more than three decades, Dr. Klevay has been a champion of the copper deficiency theory of cardiovascular disease. According to him, copper deficiency is the only single intervention that has caused the full spectrum of human cardiovascular disease in animals, including:
- Heart attacks (myocardial infarction)
- Blood clots in the coronary arteries and heart
- Fibrous atherosclerosis including smooth muscle proliferation
- Unstable blood vessel plaque
- Foam cell accumulation and fatty streaks
- Calcification of heart tissues
- Aneurysms (ruptured vessels)
- Abnormal electrocardiograms
- High cholesterol
- High blood pressure
The second reason you may not have heard of the theory is due to a lab assay called copper-mediated LDL oxidation. Researchers take LDL particles (from blood, the same ones the doctor measures as part of a cholesterol test) and expose them to a high concentration of copper in a test tube. Free copper ions are oxidants, and the researchers then measure the amount of time it takes the LDL to oxidize. I find this assay tiresome, because studies have shown that the amount of time it takes copper to oxidize LDL in a test tube doesn't predict how much oxidized LDL you'll actually find in the bloodstream of the person you took the LDL from (10, 11).
In other words, it's an assay that has little bearing on real life. But researchers like it because for some odd reason, feeding a person saturated fat causes their LDL to be oxidized more rapidly by copper in a test tube, even though that's not the case in the actual bloodstream (12). Guess which result got emphasized?
The fact that copper is such an efficient oxidant has led some researchers to propose that copper oxidizes LDL in human blood, and therefore dietary copper may contribute to heart disease (oxidized LDL is a central player in heart disease-- read more here). The problem with this theory is that there are virtually zero free copper ions in human serum. Then there's the fact that supplementing humans with copper actually reduces the susceptibility of red blood cells to oxidation (by copper in a test tube, unfortunately), which is difficult to reconcile with the idea that dietary copper increases oxidative stress in the blood (13).
The third reason you may never have heard of the theory is more problematic. Several studies have found that a higher level copper in the blood correlates with a higher risk of heart attack (14, 15). At this point, I could hang up my hat, and declare the animal experiments irrelevant to humans. But let's dig deeper.
Nutrient status is sometimes a slippery thing to measure. As it turns out, serum copper isn't a good marker of copper status. In a 4-month trial of copper depletion in humans, blood copper stayed stable, while the activity of copper-dependent enzymes in the blood declined (16). These include the important copper-dependent antioxidant, superoxide dismutase. As a side note, lysyl oxidase is another copper-dependent enzyme that cross-links the important structural proteins collagen and elastin in the artery wall, potentially explaining some of the vascular consequences of copper deficiency. Clotting factor VIII increased dramatically during copper depletion, perhaps predicting an increased tendency to clot. Even more troubling, three of the 12 women developed heart problems during the trial, which the authors felt was unusual:
We observed a significant increase over control values in the number of ventricular premature discharges (VPDs) in three women after 21, 63, and 91 d of consuming the low-copper diet; one was subsequently diagnosed as having a second-degree heart block.In another human copper restriction trial, 11 weeks of modest copper restriction coincided with heart trouble in 4 out of 23 subjects, including one heart attack (17):
In the history of conducting numerous human studies at the Beltsville Human Nutrition Research Center involving participation by 337 subjects, there had previously been no instances of any health problem related to heart function. During the 11 wk of the present study in which the copper density of the diets fed the subjects was reduced from the pretest level of 0.57 mg/ 1000 kcal to 0.36 mg/1000 kcal, 4 out of 23 subjects were diagnosed as having heart-related abnormalities.The other reason to be skeptical of the association between blood copper and heart attack risk is that inflammation increases copper in the blood (18, 19). Blood copper level correlates strongly with the marker of inflammation C-reactive protein (CRP) in humans, yet substantially increasing copper intake doesn't increase CRP (20, 21). This suggests that elevated blood copper is likely a symptom of inflammation, rather than its cause, and presents an explanation for the association between blood copper level and heart attack risk.
Only a few studies have looked at the relationship between more accurate markers of copper status and cardiovascular disease in humans. Leukocyte copper status, a marker of tissue status, is lower in people with cardiovascular disease (22, 23). People who die of heart attacks generally have less copper in their hearts than people who die of other causes, although this could be an effect rather than a cause of the heart attack (24). Overall, I find the human data lacking. I'd like to see more studies examining liver copper status in relation to cardiovascular disease, as the liver is the main storage organ for copper.
According to a 2001 study, the majority of Americans may have copper intakes below the USDA recommended daily allowance (25), many substantially so. This problem is exacerbated by the fact that copper levels in food have declined in industrial nations over the course of the 20th century, something I'll discuss in the next post.
Sunday, April 4, 2010
Magnesium and Vitamin D Metabolism
Ted Hutchinson posted a link in the comments section of my last post, pointing to a page on the Vitamin D Council's website where Dr. John Cannell discusses cofactors required for proper vitamin D metabolism. It's actually the site's home page, highlighting how important he feels this matter is. In this case, 'cofactor' simply means another nutrient that's required for the efficient production and use of vitamin D. They include:
The bottom line is that no nutrient acts in a vacuum. The effect of every part of one's diet and lifestyle is dependent on every other part. I often talk about single nutrients on this blog, but my core philosophy is that a proper diet focuses on Real Food, not nutrients. Tinkering with nutritional status using supplements is potentially problematic. Despite what some people might tell you, our understanding of nutrition and human health is currently rather crude-- so it's best to respect the accumulated wisdom of cultures that don't get the diseases we're trying to avoid.
- Magnesium
- Zinc
- Vitamin K2
- Vitamin A
- Boron
Magnesium... is essential for the normal function of the parathyroid glands, metabolism of vitamin D and adequate sensitivity of target tissues to [parathyroid hormone] and active vitamin D metabolites. Magnesium deficit is usually associated with hypoparathyroidism, low production of active vitamin D metabolites, in particular 1,25(OH)2 vitamin D3 and resistance to PTH and vitamin D. On the contrary, magnesium excess, similar to calcium, inhibits PTH secretion. Bone metabolism is impaired under positive as well as under negative magnesium balance.Magnesium status is critical for normal vitamin D metabolism, insulin sensitivity, and overall health. Supplemental magnesium blocks atherosclerosis in multiple animal models (3, 4). Most Americans don't get enough magnesium (5).
The bottom line is that no nutrient acts in a vacuum. The effect of every part of one's diet and lifestyle is dependent on every other part. I often talk about single nutrients on this blog, but my core philosophy is that a proper diet focuses on Real Food, not nutrients. Tinkering with nutritional status using supplements is potentially problematic. Despite what some people might tell you, our understanding of nutrition and human health is currently rather crude-- so it's best to respect the accumulated wisdom of cultures that don't get the diseases we're trying to avoid.
Friday, April 2, 2010
Low Vitamin D: Cause or Result of Disease?
Don Matesz at Primal Wisdom put up a post a few days ago that I think is worth reading. It follows an e-mail discussion between us concerning a paper on magnesium restriction in rats (executive summary: moderate Mg restriction reduces the hormone form of vitamin D by half and promotes osteoporosis). In his post, Don cites several papers showing that vitamin D metabolism is influenced by more than just vitamin D intake from the diet and synthesis in the skin.
Celiac disease patients have low 25(OH)D3, the circulating storage form of vitamin D, which spontaneously corrects on a gluten-free diet. There are numerous suggestions in the medical literature that overweight and sickness cause low vitamin D, potentially confounding the interpretation of studies that find lower levels of illness among people with low vitamin D levels.
Don't get me wrong, I still think vitamin D is important in preventing disease. But it does lead me to question the idea that we should force down huge doses of supplemental vitamin D to get our 25(OH)D3 up to 60, 70 or even 80 ng/mL. When the dosage of supplemental D goes beyond what a tan Caucasian could conceivably make on a day at the beach (4,000 IU?), that's when I start becoming skeptical. Check out Don's post for more.
Celiac disease patients have low 25(OH)D3, the circulating storage form of vitamin D, which spontaneously corrects on a gluten-free diet. There are numerous suggestions in the medical literature that overweight and sickness cause low vitamin D, potentially confounding the interpretation of studies that find lower levels of illness among people with low vitamin D levels.
Don't get me wrong, I still think vitamin D is important in preventing disease. But it does lead me to question the idea that we should force down huge doses of supplemental vitamin D to get our 25(OH)D3 up to 60, 70 or even 80 ng/mL. When the dosage of supplemental D goes beyond what a tan Caucasian could conceivably make on a day at the beach (4,000 IU?), that's when I start becoming skeptical. Check out Don's post for more.
Thursday, March 25, 2010
Interesting Articles in the AJCN
I just received an RSS alert for the American Journal of Clinical Nutrition's latest articles. This upcoming issue is full of very interesting material:
1. Dr. Neil D. Barnard reviews food consumption patterns in the US from 1909 to 2007 (1). This is something I've written about a number of times. The most notable change is that industrial seed oil use has increased by more than 3-fold in the last 40 years, and even more in the last 100 although he doesn't provide those numbers. Butter and lard use declined sharply. Meat consumption is up, but the increase comes exclusively from poultry because we're eating the same amount of red meat we always have. Grain consumption is down, although it peaked around 1900 so it may not be a fair comparison with today:
3. Soy protein and isoflavones, which have been proposed to do everything from increase bone mineral density to fight cancer, are slowly falling out of favor. Dr. Z.M. Liu and colleagues show that soy protein and/or isoflavone supplementation has no effect on insulin sensitivity or glucose tolerance in a 6 month trial (3). This follows a recent trial showing that isoflavones have no effect on bone mineral density.
4. Dr. Ines Birlouez-Aragon and colleagues showed that high-heat cooked (fried and sauteed) foods increase risk factors for diabetes and cardiovascular disease (insulin resistance, cholesterol, triglycerides), compared to low-heat cooked foods (steamed, stewed) in a one-month trial (4). The high-heat diet also reduced serum levels of long-chain omega-3 fatty acids and vitamins C and E.
5. Dr. Katharina Nimptsch and colleagues showed that higher menaquinone (vitamin K2) intake is associated with a lower cancer incidence and lower cancer mortality in Europeans (5). Most of their K2 came from cheese.
6. And finally, Dr. Zhaoping Li and colleagues showed that cooking meat with an herb and spice blend reduced the levels of oxidized fat during cooking, and reduced serum and urinary markers of lipid oxidation in people eating the meat (6).
The take-home message? Eat stewed beef with herbs, but don't pre-brown it in vegetable oil. Throw out the tofu and have some artisanal cheese instead.
1. Dr. Neil D. Barnard reviews food consumption patterns in the US from 1909 to 2007 (1). This is something I've written about a number of times. The most notable change is that industrial seed oil use has increased by more than 3-fold in the last 40 years, and even more in the last 100 although he doesn't provide those numbers. Butter and lard use declined sharply. Meat consumption is up, but the increase comes exclusively from poultry because we're eating the same amount of red meat we always have. Grain consumption is down, although it peaked around 1900 so it may not be a fair comparison with today:
In the late 1800s, wheat flours became more popular and available due to the introduction of new [high-gluten] wheat varieties, [low extraction] milling techniques, and transport methods, and during this time new breakfast cereals were introduced by John Harvey Kellogg, CW Post, and the Quaker Oats Company. Thereafter, however, per capita availability of flour and cereal products gradually dropped as increased prosperity, improved mechanization, and transport (eg, refrigerated railway cars) increased competition from other food groups. [Then they partially rebounded in the last 40 years]2. Dr. S.C. Larsson published a paper showing that in Sweden, multivitamin use is associated with a slightly higher risk of breast cancer (2).
3. Soy protein and isoflavones, which have been proposed to do everything from increase bone mineral density to fight cancer, are slowly falling out of favor. Dr. Z.M. Liu and colleagues show that soy protein and/or isoflavone supplementation has no effect on insulin sensitivity or glucose tolerance in a 6 month trial (3). This follows a recent trial showing that isoflavones have no effect on bone mineral density.
4. Dr. Ines Birlouez-Aragon and colleagues showed that high-heat cooked (fried and sauteed) foods increase risk factors for diabetes and cardiovascular disease (insulin resistance, cholesterol, triglycerides), compared to low-heat cooked foods (steamed, stewed) in a one-month trial (4). The high-heat diet also reduced serum levels of long-chain omega-3 fatty acids and vitamins C and E.
5. Dr. Katharina Nimptsch and colleagues showed that higher menaquinone (vitamin K2) intake is associated with a lower cancer incidence and lower cancer mortality in Europeans (5). Most of their K2 came from cheese.
6. And finally, Dr. Zhaoping Li and colleagues showed that cooking meat with an herb and spice blend reduced the levels of oxidized fat during cooking, and reduced serum and urinary markers of lipid oxidation in people eating the meat (6).
The take-home message? Eat stewed beef with herbs, but don't pre-brown it in vegetable oil. Throw out the tofu and have some artisanal cheese instead.
Tuesday, March 23, 2010
New Review of Controlled Trials Replacing Saturated fat with Industrial Seed Oils
Readers Stanley and JBG just informed me of a new review paper by Dr. Dariush Mozaffarian and colleagues. Dr. Mozaffarian is one of the Harvard epidemiologists responsible for the Nurse's Health study. The authors claim that overall, the controlled trials show that replacing saturated fat with polyunsaturated fat from industrial seed oils, but not carbohydrate or monounsaturated fat (as in olive oil), slightly reduces the risk of having a heart attack:
So basically, even if the authors' conclusion were correct, you overhaul your whole diet and replace natural foods with bland unnatural foods, and...? You reduce your 10-year risk of having a heart attack from 10 percent to 9 percent. Without affecting your overall risk of dying! The paper states that the interventions didn't affect overall mortality at all. That's what they're talking about here. Sign me up!
* Autopsies were not conducted in a blinded manner. Physicians knew which hospital the cadavers came from, because autopsies were done on-site. There is some confusion about this point because the second paper states that physicians interpreted the autopsy reports in a blinded manner. But that doesn't make it blinded, since the autopsies weren't blinded. The patients were also not blinded, so the study overall was highly susceptible to bias.
** They refer to it as "cluster randomized". I don't know if that term accurately applies to the Finnish trial or not. The investigators definitely didn't randomize the individual patients: whichever hospital a person was being treated in, that's the food he/she ate. There were only two hospitals, so "cluster randomization" in this case would just refer to deciding which hospital got the intervention first. Can this accurately be called randomized?
These findings provide evidence that consuming PUFA in place of SFA reduces CHD events in RCTs [how do you like the acronyms?]. This suggests that rather than trying to lower PUFA consumption, a shift toward greater population PUFA consumption in place of SFA would significantly reduce rates of CHD.Looking at the studies they included in their analysis (and at those they excluded), it looks like they did a very nice job cherry picking. For example:
- They included the Finnish Mental Hospital trial, which is a terrible trial for a number of reasons. It wasn't randomized, appropriately controlled or even semi-blinded*. Thus, it doesn't fit the authors' stated inclusion criteria, but they included it in their analysis anyway**. Besides, the magnitude of the result has never been replicated by better trials, not even close.
- They included two trials that changed more than just the proportion of SFA to PUFA. For example, the Oslo Diet-heart trial replaced animal fat with seed oils, but also increased fruit, nut, vegetable and fish intake, while reducing trans fat margarine intake! The STARS trial increased both omega-6 and omega-3, reduced processed food intake, and increased fruit and vegetable intake! These obviously aren't controlled trials isolating the issue of dietary fat substitution. If you subtract the four inappropriate trials from their analysis, which is half the studies they analyzed, the result disappears. Those four just happened to show the largest reduction in heart attack mortality...
- They excluded the Rose et al. corn oil trial and the Sydney Diet-heart trial. Both found a large increase in total mortality from replacing animal fat with seed oils, and the Rose trial found a large increase in heart attack deaths (the Sydney trial didn't report CHD deaths, but Dr. Mozaffarian et al. stated in their paper that they contacted authors to obtain unpublished results. Why didn't they contact the authors of this study?).
So basically, even if the authors' conclusion were correct, you overhaul your whole diet and replace natural foods with bland unnatural foods, and...? You reduce your 10-year risk of having a heart attack from 10 percent to 9 percent. Without affecting your overall risk of dying! The paper states that the interventions didn't affect overall mortality at all. That's what they're talking about here. Sign me up!
* Autopsies were not conducted in a blinded manner. Physicians knew which hospital the cadavers came from, because autopsies were done on-site. There is some confusion about this point because the second paper states that physicians interpreted the autopsy reports in a blinded manner. But that doesn't make it blinded, since the autopsies weren't blinded. The patients were also not blinded, so the study overall was highly susceptible to bias.
** They refer to it as "cluster randomized". I don't know if that term accurately applies to the Finnish trial or not. The investigators definitely didn't randomize the individual patients: whichever hospital a person was being treated in, that's the food he/she ate. There were only two hospitals, so "cluster randomization" in this case would just refer to deciding which hospital got the intervention first. Can this accurately be called randomized?
Saturday, March 20, 2010
Fatty Liver: It's not Just for Grown-ups Anymore
The epidemic of non-alcoholic fatty liver disease (NAFLD) is one of my favorite topics on this blog, due to the liver's role as the body's metabolic "grand central station", as Dr. Philip Wood puts it. The liver plays a critical part in the regulation of sugar, insulin, and lipid levels in the blood. Many of the routine blood tests administered in the doctor's office (blood glucose, cholesterol, etc.) partially reflect liver function.
NAFLD is an excessive accumulation of fat in the liver that impairs its function and can lead to severe liver inflammation (NASH), and in a small percentage of people, liver cancer. An estimated 20-30% of people in industrial nations suffer from NAFLD, a shockingly high prevalence (1).
I previously posted on dietary factors I believe are involved in NAFLD. In rodents, feeding a large amount of sugar or industrial seed oils (corn oil, etc.) promotes NAFLD, whereas fats such as butter and coconut oil do not (2). In human infants, enteric feeding with industrial seed oils causes severe liver damage, whereas the same amount of fat from fish oil doesn't, and can even reverse the damage done by seed oils (3).
So basically, I think sugar and industrial oils are major contributors to NAFLD, and if you look at diet trends in the US over the last 40 years, they're consistent with the idea. Industrial oils are harmful due (at least in part) to their high omega-6 content, which is problematic partially because it disturbs normal omega-3 metabolism. A potential solution to fatty liver is to reduce sugar, replace industrial oils with natural fats, and ensure a regular source of omega-3. I've posted two anecdotes of people rapidly healing their fatty livers using diet changes* (4, 5).
I recently came across a study that examined the diet of Canadian children with NAFLD (6). The children had a high sugar intake, a typical (i.e., high) omega-6 intake, and a low omega-3 intake. The authors claimed that the children also had a high saturated fat intake, but at 10.5% of calories, they were almost eating to the American Heart Association's "Step I" diet recommendations**. Busted! Total fat intake was also low.
High sugar consumption was associated with a larger waist circumference, insulin resistance, lower adiponectin and elevated markers of inflammation. High omega-6 intake was associated with markers of inflammation. Low omega-3 intake was associated with insulin resistance and elevated liver enzymes. Saturated fat intake presumably had no relation to any of these markers, since they didn't mention it in the text.
These children with NAFLD, who were all insulin resistant and mostly obese, had diets high in omega-6, high in sugar, and low in omega-3. This is consistent with the idea that these three factors, which have all been moving in the wrong direction in the last 40 years, contribute to NAFLD.
* Fatty liver was assessed by liver enzymes, admittedly not a perfect test. However, elevated liver enzymes do correlate fairly well with NAFLD.
** Steps I and II were replaced by new diet advice in 2000. The AHA now recommends keeping saturated fat below 7% of calories. Stock up on those skinless chicken breasts! Make sure there isn't any residual fat sticking to the meat, it might kill you. I do have to give the AHA credit however, because their new recommendations focus mostly on eating real food rather than avoiding saturated fat and cholesterol.
NAFLD is an excessive accumulation of fat in the liver that impairs its function and can lead to severe liver inflammation (NASH), and in a small percentage of people, liver cancer. An estimated 20-30% of people in industrial nations suffer from NAFLD, a shockingly high prevalence (1).
I previously posted on dietary factors I believe are involved in NAFLD. In rodents, feeding a large amount of sugar or industrial seed oils (corn oil, etc.) promotes NAFLD, whereas fats such as butter and coconut oil do not (2). In human infants, enteric feeding with industrial seed oils causes severe liver damage, whereas the same amount of fat from fish oil doesn't, and can even reverse the damage done by seed oils (3).
So basically, I think sugar and industrial oils are major contributors to NAFLD, and if you look at diet trends in the US over the last 40 years, they're consistent with the idea. Industrial oils are harmful due (at least in part) to their high omega-6 content, which is problematic partially because it disturbs normal omega-3 metabolism. A potential solution to fatty liver is to reduce sugar, replace industrial oils with natural fats, and ensure a regular source of omega-3. I've posted two anecdotes of people rapidly healing their fatty livers using diet changes* (4, 5).
I recently came across a study that examined the diet of Canadian children with NAFLD (6). The children had a high sugar intake, a typical (i.e., high) omega-6 intake, and a low omega-3 intake. The authors claimed that the children also had a high saturated fat intake, but at 10.5% of calories, they were almost eating to the American Heart Association's "Step I" diet recommendations**. Busted! Total fat intake was also low.
High sugar consumption was associated with a larger waist circumference, insulin resistance, lower adiponectin and elevated markers of inflammation. High omega-6 intake was associated with markers of inflammation. Low omega-3 intake was associated with insulin resistance and elevated liver enzymes. Saturated fat intake presumably had no relation to any of these markers, since they didn't mention it in the text.
These children with NAFLD, who were all insulin resistant and mostly obese, had diets high in omega-6, high in sugar, and low in omega-3. This is consistent with the idea that these three factors, which have all been moving in the wrong direction in the last 40 years, contribute to NAFLD.
* Fatty liver was assessed by liver enzymes, admittedly not a perfect test. However, elevated liver enzymes do correlate fairly well with NAFLD.
** Steps I and II were replaced by new diet advice in 2000. The AHA now recommends keeping saturated fat below 7% of calories. Stock up on those skinless chicken breasts! Make sure there isn't any residual fat sticking to the meat, it might kill you. I do have to give the AHA credit however, because their new recommendations focus mostly on eating real food rather than avoiding saturated fat and cholesterol.
Wednesday, March 17, 2010
Book Review: The Primal Blueprint
Mark Sisson has been a central figure in the evolutionary health community since he began his weblog Mark's Daily Apple in 2006. He and his staff have been posting daily on his blog ever since. He has also written several other books, edited the Optimum Health newsletter, competed as a high-level endurance athlete, and served on the International Triathlon Union as the anti-doping chairman, all of which you can read about on his biography page. Mark is a practice-what-you-preach kind of guy, and if physical appearance means anything, he's on to something.
In 2009, Mark published his long-awaited book The Primal Blueprint. He self-published the book, which has advantages and disadvantages. The big advantage is that you aren't subject to the sometimes onerous demands of publishers, who attempt to maximize sales at Barnes and Noble. The front cover sports a simple picture of Mark, rather than a sunbaked swimsuit model, and the back cover offers no ridiculous claims of instant beauty and fat loss.
The drawback of self-publishing is it's more difficult to break into a wider market. That's why Mark has asked me to publish my review of his book today. He's trying to push it up in the Amazon.com rankings so that it gets a broader exposure. If you've been thinking about buying Mark's book, now is a good time to do it. If you order it from Amazon.com on March 17th, Mark is offering to sweeten the deal with some freebies on his site Mark's Daily Apple. Full disclosure: I'm not getting anything out of this, I'm simply mentioning it because I was reviewing Mark's book anyway and I thought some readers might enjoy it.
The Primal Blueprint is not a weight loss or diet book, it's a lifestyle program with an evolutionary slant. Mark uses the example of historical and contemporary hunter-gatherers as a model, and attempts to apply those lessons to life in the 21st century. He does it in a way that's empowering accessible to nearly everyone. To illustrate his points, he uses the example of an archetypal hunter-gatherer called Grok, and his 21st century mirror image, the Korg family.
The diet section will be familiar to anyone who has read about "paleolithic"-type diets. He advocates eating meats including organs, seafood, eggs, nuts, abundant vegetables, and fruit. He also suggests avoiding grains, legumes, dairy (although he's not very militant about this one), processed food in general, and reducing carbohydrate to less than 150 grams per day. I like his diet suggestions because they focus on real food. Mark is not a drill sergeant. He tries to create a plan that will be sustainable in the long run, by staying positive and allowing for cheats.
We part ways on the issue of carbohydrate. He suggests that eating more than 150 grams of carbohydrate per day leads to fat gain and disease, whereas I feel that position is untenable in light of what we know of non-industrial cultures (including some relatively high-carbohydrate hunter-gatherers). Although carbohydrate restriction (or at least wheat and sugar restriction) does have its place in treating obesity and metabolic dysfunction in modern populations, ultimately I don't think it's necessary for the prevention of those same problems, and it can even be counterproductive in some cases. Mark does acknowledge that refined carbohydrates are the main culprits.
The book's diet section also recommends nutritional supplements, including a multivitamin/mineral, antioxidant supplement, probiotics, protein powder and fish oil. I'm not a big proponent of supplementation. I'm also a bit of a hypocrite because I do take small doses of fish oil (when I haven't had seafood recently), and vitamin D in wintertime. But I can't get behind protein powders and antioxidant supplements.
Mark's suggestions for exercise, sun exposure, sleep and stress management make good sense to me. In a nutshell: do all three, but keep the exercise varied and don't overdo it. As a former high-level endurance athlete, he has a lot of credibility here. He puts everything in a format that's practical, accessible and empowering.
I think The Primal Blueprint is a useful book for a person who wants to maintain or improve her health. Although we disagree on the issue of carbohydrate, the diet and lifestyle advice is solid and will definitely be a vast improvement over what the average person is doing. The Primal Blueprint is not an academic book, nor does it attempt to be. It doesn't contain many references (although it does contain some), and it won't satisfy someone looking for an in-depth discussion of the scientific literature. However, it's perfect for someone who's getting started and needs guidance, or who simply wants a more comprehensive source than reading blog snippets. It would make a great gift for that family member or friend who's been asking how you stay in such good shape.
In 2009, Mark published his long-awaited book The Primal Blueprint. He self-published the book, which has advantages and disadvantages. The big advantage is that you aren't subject to the sometimes onerous demands of publishers, who attempt to maximize sales at Barnes and Noble. The front cover sports a simple picture of Mark, rather than a sunbaked swimsuit model, and the back cover offers no ridiculous claims of instant beauty and fat loss.
The drawback of self-publishing is it's more difficult to break into a wider market. That's why Mark has asked me to publish my review of his book today. He's trying to push it up in the Amazon.com rankings so that it gets a broader exposure. If you've been thinking about buying Mark's book, now is a good time to do it. If you order it from Amazon.com on March 17th, Mark is offering to sweeten the deal with some freebies on his site Mark's Daily Apple. Full disclosure: I'm not getting anything out of this, I'm simply mentioning it because I was reviewing Mark's book anyway and I thought some readers might enjoy it.
The Primal Blueprint is not a weight loss or diet book, it's a lifestyle program with an evolutionary slant. Mark uses the example of historical and contemporary hunter-gatherers as a model, and attempts to apply those lessons to life in the 21st century. He does it in a way that's empowering accessible to nearly everyone. To illustrate his points, he uses the example of an archetypal hunter-gatherer called Grok, and his 21st century mirror image, the Korg family.
The diet section will be familiar to anyone who has read about "paleolithic"-type diets. He advocates eating meats including organs, seafood, eggs, nuts, abundant vegetables, and fruit. He also suggests avoiding grains, legumes, dairy (although he's not very militant about this one), processed food in general, and reducing carbohydrate to less than 150 grams per day. I like his diet suggestions because they focus on real food. Mark is not a drill sergeant. He tries to create a plan that will be sustainable in the long run, by staying positive and allowing for cheats.
We part ways on the issue of carbohydrate. He suggests that eating more than 150 grams of carbohydrate per day leads to fat gain and disease, whereas I feel that position is untenable in light of what we know of non-industrial cultures (including some relatively high-carbohydrate hunter-gatherers). Although carbohydrate restriction (or at least wheat and sugar restriction) does have its place in treating obesity and metabolic dysfunction in modern populations, ultimately I don't think it's necessary for the prevention of those same problems, and it can even be counterproductive in some cases. Mark does acknowledge that refined carbohydrates are the main culprits.
The book's diet section also recommends nutritional supplements, including a multivitamin/mineral, antioxidant supplement, probiotics, protein powder and fish oil. I'm not a big proponent of supplementation. I'm also a bit of a hypocrite because I do take small doses of fish oil (when I haven't had seafood recently), and vitamin D in wintertime. But I can't get behind protein powders and antioxidant supplements.
Mark's suggestions for exercise, sun exposure, sleep and stress management make good sense to me. In a nutshell: do all three, but keep the exercise varied and don't overdo it. As a former high-level endurance athlete, he has a lot of credibility here. He puts everything in a format that's practical, accessible and empowering.
I think The Primal Blueprint is a useful book for a person who wants to maintain or improve her health. Although we disagree on the issue of carbohydrate, the diet and lifestyle advice is solid and will definitely be a vast improvement over what the average person is doing. The Primal Blueprint is not an academic book, nor does it attempt to be. It doesn't contain many references (although it does contain some), and it won't satisfy someone looking for an in-depth discussion of the scientific literature. However, it's perfect for someone who's getting started and needs guidance, or who simply wants a more comprehensive source than reading blog snippets. It would make a great gift for that family member or friend who's been asking how you stay in such good shape.
Saturday, March 13, 2010
Interview on Bizymoms
I recently did a written interview for the website Bizymoms.com. It was the first time I had been invited to do an interview, so I figured what the heck. They bravely posted the interview, despite the fact that my responses could be seen as controversial. You can find it here.
Thursday, March 11, 2010
Vitamin D May Prevent Flu and Asthma
The AJCN just published a new controlled trial evaluating the effectiveness of vitamin D supplements on flu and asthma (1). Dr. Hiroyuki Ida's group gave Japanese schoolchildren (10 years average age) 1,200 IU of vitamin D3 or placebo per day from December through March. They found that children taking vitamin D had a significantly lower incidence of influenza A but not influenza B. These are two strains of flu that each accounted for roughly half the flu incidence in this population. Sadly, if you add the total flu incidence for A and B together (which the authors don't do in their tables), vitamin D supplementation didn't reduce total flu incidence significantly.
They also found that in the subset of children not already taking vitamin D supplements, the effect was greater, with unsupplemented children contracting nearly three times as many influenza A infections as children receiving vitamin D. They didn't analyze the influenza B or total influenza incidence in that way, so we don't know if prior supplementation makes a difference there.
The most striking finding of the paper is that the vitamin D group suffered from 6 times fewer asthma attacks than the placebo group. This needs to be repeated but it's consistent with other data and I find it very encouraging.
The paper did have some limitations. They didn't measure vitamin D status so they have no way to know exactly how effective their pill-based supplements were.
Another problem is that they began collecting data immediately after beginning supplementation. Vitamin D is a fat-soluble vitamin that can take 3 months to reach maximum concentration in the body following supplementation. By the time the children were reaching their maximum serum concentration of vitamin D, the trial was over. It would be nice to see the next trial begin supplementation in the fall and look at flu incidence in the winter.
This paper comes on the heels of another showing that vitamin D is necessary for the activation of an immune cell called the killer T cell (2). These are important for resistance to infections and cancer. Overall, these papers add to the accumulating evidence that vitamin D is important for the proper functioning of the human immune system. However, mice may not be the best model for use in studying vitamin D biology. From the first paper:
They also found that in the subset of children not already taking vitamin D supplements, the effect was greater, with unsupplemented children contracting nearly three times as many influenza A infections as children receiving vitamin D. They didn't analyze the influenza B or total influenza incidence in that way, so we don't know if prior supplementation makes a difference there.
The most striking finding of the paper is that the vitamin D group suffered from 6 times fewer asthma attacks than the placebo group. This needs to be repeated but it's consistent with other data and I find it very encouraging.
The paper did have some limitations. They didn't measure vitamin D status so they have no way to know exactly how effective their pill-based supplements were.
Another problem is that they began collecting data immediately after beginning supplementation. Vitamin D is a fat-soluble vitamin that can take 3 months to reach maximum concentration in the body following supplementation. By the time the children were reaching their maximum serum concentration of vitamin D, the trial was over. It would be nice to see the next trial begin supplementation in the fall and look at flu incidence in the winter.
This paper comes on the heels of another showing that vitamin D is necessary for the activation of an immune cell called the killer T cell (2). These are important for resistance to infections and cancer. Overall, these papers add to the accumulating evidence that vitamin D is important for the proper functioning of the human immune system. However, mice may not be the best model for use in studying vitamin D biology. From the first paper:
The evolution of different mechanisms for the regulation of PLC-γ1 activity in human and mouse T cells parallels the development of divergent VDR-dependent and VDR-independent antimicrobial pathways in human and mouse macrophages31, respectively, and may reflect the fact that mice are nocturnal animals with fur and humans are daytime creatures that synthesize vitamin D in the skin after exposure to ultraviolet light.In other words, mice don't use vitamin D in the same way as humans because they have a different evolutionary relationship to it.
Wednesday, March 10, 2010
A False Dichotomy
In the discussion section of the last post, the eternal argument about non-industrial people arose: were their lives (a) "nasty, brutish and short" (Hobbes), or were they (b) "noble savages" (Shaftesbury) living in Eden? The former argument states that they had awful lives, and we should be glad we're living int he 21st century. The latter argument implies that we should emulate them as much as possible. Each side is bursting with anecdotes to support their position.
Any time the discussion reaches this point, it stops providing us anything useful. The argument is a false dichotomy, one in which neither answer is correct. The correct answer is (c): none of the above. Some aspects of hunter-gatherer life are preferable to ours, and some aspects of our lives are preferable to theirs. Understanding that we spent a lot of evolutionary time as hunter-gatherers, as well as a few thousand years in small, tightly knit agricultural communities, may be useful in understanding how to work constructively with our own bodies and minds in the modern world.
So please, let's leave behind the false dichotomy and foster a more nuanced understanding of hunter-gatherer life.
Any time the discussion reaches this point, it stops providing us anything useful. The argument is a false dichotomy, one in which neither answer is correct. The correct answer is (c): none of the above. Some aspects of hunter-gatherer life are preferable to ours, and some aspects of our lives are preferable to theirs. Understanding that we spent a lot of evolutionary time as hunter-gatherers, as well as a few thousand years in small, tightly knit agricultural communities, may be useful in understanding how to work constructively with our own bodies and minds in the modern world.
So please, let's leave behind the false dichotomy and foster a more nuanced understanding of hunter-gatherer life.
Monday, March 8, 2010
The Paleolithic Mind
I went to a meditation retreat this week with the Red Cedar Zen community in Bellingham. It was a good experience. Staring at a wall from 6 am to 9 pm for a few days gives you the opportunity to learn a few things about your mind. Some of these are things you already know on some level, but you just need to have them reinforced. For example, the weight of psychological stress that we carry in modern societies like the US. It's only when it goes away for a while that you can see how heavy it was.
I'm totally ignorant of the scientific literature on this, but the way I see it, there are at least two main sources of psychological stress in the modern world for which we aren't well equipped as human beings:
The author says this about their possessions:
Unfortunately, we have more than just possessions on our minds. To live in the modern world is to be pricked to death by a thousand small responsibilities. Remember to make your lunch. Remember to make a doctor's appointment, shop for groceries, tie your shoes, get your oil changed, send that e-mail, make dinner, go for a jog, vacuum the floor, take a shower, pick up the kids-- the list is endless. Are our memories as defective as we think they are, or are we simply not designed to keep track of so many details?
In hunter-gatherer times, we had stress. Homicide, accidents, infectious disease and predation were always stalking us. But it was a totally different kind of stress-- it was occasional, powerful and brief rather than a constant flow of obligations clogging the paths of our minds. Most days were leisurely, with plenty of time for gossiping, staring at the clouds and dozing off.
Those times are gone for us, but perhaps keeping them in mind can help us live more constructively in the modern world. I find that meditation helps keep the thousand pricks of modern life in perspective, perhaps bringing my mind closer to the paleolithic state.
I'm totally ignorant of the scientific literature on this, but the way I see it, there are at least two main sources of psychological stress in the modern world for which we aren't well equipped as human beings:
- Being eternally and inescapably subordinate in a large social structure
- Having too many responsibilities such as possessions and obligations
The Hadza do not engage in warfare [although they do have homicide]. They've never lived densely enough to be seriously threatened by an infectious outbreak. They have no known history of famine; rather, there is evidence of people from a farming group coming to live with them during a time of crop failure. The Hadza diet remains even today more stable and varied than that of most of the world's citizens. They enjoy an extraordinary amount of leisure time. Anthropologists have estimated that they "work"—actively pursue food—four to six hours a day. And over all these thousands of years, they've left hardly more than a footprint on the land.This isn't intended to idealize their lifestyle, but to point out that being a hunter-gatherer has its advantages. One of these is a minimal social structure in which each person is has full authority over himself:
The Hadza recognize no official leaders. Camps are traditionally named after a senior male (hence, Onwas's camp), but this honor does not confer any particular power. Individual autonomy is the hallmark of the Hadza. No Hadza adult has authority over any other. None has more wealth; or, rather, they all have no wealth. There are few social obligations—no birthdays, no religious holidays, no anniversaries.Even "marriage" doesn't carry much obligation. The author describes the Hadza as "serial monogamists". The idea of an eternal bond between two individuals doesn't exist. Women are not subordinate to men:
Gender roles are distinct, but for women there is none of the forced subservience knit into many other cultures. A significant number of Hadza women who marry out of the group soon return, unwilling to accept bullying treatment. Among the Hadza, women are frequently the ones who initiate a breakup—woe to the man who proves himself an incompetent hunter or treats his wife poorly. In Onwas's camp, some of the loudest, brashest members were women.Contrast this with modern civilizations in which everyone has a boss-- whether it's at a job, in a marriage or under your country's legal system. I think this feeling of perpetual subordination is destructive to an animal such as ourselves, that has spent so much of its existence mostly free of these pressures.
The author says this about their possessions:
Traditional Hadza, like Onwas and his camp mates, live almost entirely free of possessions. The things they own—a cooking pot, a water container, an ax—can be wrapped in a blanket and carried over a shoulder.This resembles other African hunter-gatherer groups that have few and simple tools. From the book The !Kung San: Men, Women and Work in a Foraging Society:
!Kung tools are few in number, lightweight, made from locally available materials, and multipurpose.Again, this is in sharp contrast to the modern world, where we have so many belongings it's impossible to keep track of them all. We have giant houses that we "need" to store all these things, and still it doesn't seem like enough. Many of our possessions are indispensable if we want to fit in to society. We need (or feel we need) clothes, cookware, identification, money, transportation, furniture, tools, sports gear, et cetera. Having to be responsible for this extraordinary quantity of possessions (by evolutionary standards) is a heavy weight on our minds.
Unfortunately, we have more than just possessions on our minds. To live in the modern world is to be pricked to death by a thousand small responsibilities. Remember to make your lunch. Remember to make a doctor's appointment, shop for groceries, tie your shoes, get your oil changed, send that e-mail, make dinner, go for a jog, vacuum the floor, take a shower, pick up the kids-- the list is endless. Are our memories as defective as we think they are, or are we simply not designed to keep track of so many details?
In hunter-gatherer times, we had stress. Homicide, accidents, infectious disease and predation were always stalking us. But it was a totally different kind of stress-- it was occasional, powerful and brief rather than a constant flow of obligations clogging the paths of our minds. Most days were leisurely, with plenty of time for gossiping, staring at the clouds and dozing off.
Those times are gone for us, but perhaps keeping them in mind can help us live more constructively in the modern world. I find that meditation helps keep the thousand pricks of modern life in perspective, perhaps bringing my mind closer to the paleolithic state.
Monday, March 1, 2010
Book Review: S.P.E.E.D.
This book was sent to me by Matt Schoeneberger, who co-authored it with Jeff Thiboutot. Both have master's degrees in exercise science and health promotion. S.P.E.E.D. stands for Sleep, Psychology, Exercise, Environment and Diet. The authors have attempted to create a concise, comprehensive weight loss strategy based on what they feel is the most compelling scientific evidence available. It's subtitled "The Only Weight Loss Book Worth Reading". Despite the subtitle that's impossible to live up to, it was an interesting and well-researched book. It was a very fast read at 205 large-print pages including 32 pages of appendices and index.
I really appreciate the abundant in-text references the authors provided. I have a hard time taking a health and nutrition book seriously that doesn't provide any basis to evaluate its statements. There are already way too many people flapping their lips out there, without providing any outside support for their statements, for me to tolerate that sort of thing. Even well-referenced books can be a pain if the references aren't in the text itself. Schoeneberger and Thiboutot provided appropriate, accessible references for nearly every major statement in the book.
Chapter one, "What is a Healthy Weight", discusses the evidence for an association between body weight and health. They note that both underweight and obesity are associated with poor health outcomes, whereas moderate overweight isn't. While I agree, I continue to maintain that being fairly lean and appropriately muscled (which doesn't necessarily mean muscular) is probably optimal. The reason that people with a body mass index (BMI) considered to be "ideal" aren't healthier on average than people who are moderately overweight may have to do with the fact that many people with an "ideal" BMI are skinny-fat, i.e. have low muscle mass and too much abdominal fat.
Chapter 2, "Sleep", discusses the importance of sleep in weight regulation and overall health. They reference some good studies and I think they make a compelling case that it's important. Chapter 3, "Psychology", details psychological strategies to motivate and plan for effective weight loss.
Chapter 4, "Exercise", provides an exercise plan for weight loss. The main message: do it! I think they give a fair overview of the different categories of exercise and their relative merits, including high-intensity intermittent training (HIIT). However, the exercise regimen they suggest is intense and will probably lead to overtraining in many people. They recommend resistance training major, multi-joint exercises, 1-3 sets to muscular failure 2-4 days a week. I've been at the higher end of that recommendation and it made my joints hurt, plus I was weaker than when I strength trained less frequently. I think the lower end of their recommendation, 1 set of each exercise to failure twice a week, is more than sufficient to meet the goal of maximizing improvements in body composition in most people. My current routine is one brief strength training session and one sprint session per week (in addition to my leisurely cycle commute), which works well for me on a cost-benefit level. However, I was stronger when I was strength training twice a week and never going to muscular failure (a la Pavel Tsatsouline).
Chapter 5, "Environment", is an interesting discussion of different factors that promote excessive calorie intake, such as the setting of the meal, the company or lack thereof, and food presentation. While they support their statements very well with evidence from scientific studies, I do have a lingering doubt about these types of studies: as far as I know, they're all based on short-term interventions. Science would be a lot easier if short-term always translated to long term, but unfortunately that's not the case. For example, studies lasting one or two weeks show that low glycemic index foods cause a reduction in calorie intake and greater feelings of fullness. However, this effect disappears in the long term, and numerous controlled trials show that low glycemic index diets have no effect on food intake, body weight or insulin sensitivity in the long term. I reviewed those studies here.
The body has homeostatic mechanisms (homeostatic = maintains the status quo) that regulate long-term energy balance. Whether short-term changes in calorie intake based on environmental cues would translate into sustained changes that would have a significant impact on body fat, I don't know. For example, if you eat a meal with your extended family at a restaurant that serves massive portions, you might eat twice as much as you would by yourself in your own home. But the question is, will your body factor that huge meal into your subsequent calorie intake and energy expenditure over the following days? The answer is clearly yes, but the degree of compensation is unclear. Since I'm not aware of any trials indicating that changing meal context can actually lead to long-term weight loss, I can't put much faith in this strategy (if you know otherwise, please link to the study in the comments).
Chapter 6, "Diet", is a very brief discussion of what to eat for weight loss. They basically recommend a low-calorie, low-carb diet focused on whole, natural foods. I think low-carbohydrate diets can be useful for some overweight people trying to lose weight, if for no other reason than the fact that they make it easier to control appetite. In addition, a subset of people respond very well to carbohydrate restriction in terms of body composition, health and well-being. The authors emphasize nutrient density, but don't really explain how to achieve it. It would have been nice to see a discussion of a few topics such as organ meats, leafy greens, dairy quality (pastured vs. conventional) and vitamin D. These may not help you lose weight, but they will help keep you healthy, particularly on a calorie-restricted diet. The authors also recommend a few energy bars, powders and supplements that I don't support. They state that they have no financial connection to the manufacturers of the products they recommend.
I'm wary of their recommendation to deliberately restrict calorie intake. Although it will clearly cause fat loss if you restrict calories enough, it's been shown to be ineffective for sustainable, long-term fat loss over and over again. The only exception is the rare person with an iron will who is able to withstand misery indefinitely. I'm going to keep an open mind on this question though. There may be a place for deliberate calorie restriction in the right context. But at this point I'm going to require some pretty solid evidence that it's effective, sustainable, and doesn't have unacceptable side effects.
The book contains a nice bonus, an appendix titled "What is Quality Evidence"? It's a brief discussion of common logical pitfalls when evaluating evidence, and I think many people could benefit from reading it.
Overall, S.P.E.E.D. was a worthwhile read, definitely superior to 95% of fat loss books. With some caveats mentioned above, I think it could be a useful resource for someone interested in fat loss.
I really appreciate the abundant in-text references the authors provided. I have a hard time taking a health and nutrition book seriously that doesn't provide any basis to evaluate its statements. There are already way too many people flapping their lips out there, without providing any outside support for their statements, for me to tolerate that sort of thing. Even well-referenced books can be a pain if the references aren't in the text itself. Schoeneberger and Thiboutot provided appropriate, accessible references for nearly every major statement in the book.
Chapter one, "What is a Healthy Weight", discusses the evidence for an association between body weight and health. They note that both underweight and obesity are associated with poor health outcomes, whereas moderate overweight isn't. While I agree, I continue to maintain that being fairly lean and appropriately muscled (which doesn't necessarily mean muscular) is probably optimal. The reason that people with a body mass index (BMI) considered to be "ideal" aren't healthier on average than people who are moderately overweight may have to do with the fact that many people with an "ideal" BMI are skinny-fat, i.e. have low muscle mass and too much abdominal fat.
Chapter 2, "Sleep", discusses the importance of sleep in weight regulation and overall health. They reference some good studies and I think they make a compelling case that it's important. Chapter 3, "Psychology", details psychological strategies to motivate and plan for effective weight loss.
Chapter 4, "Exercise", provides an exercise plan for weight loss. The main message: do it! I think they give a fair overview of the different categories of exercise and their relative merits, including high-intensity intermittent training (HIIT). However, the exercise regimen they suggest is intense and will probably lead to overtraining in many people. They recommend resistance training major, multi-joint exercises, 1-3 sets to muscular failure 2-4 days a week. I've been at the higher end of that recommendation and it made my joints hurt, plus I was weaker than when I strength trained less frequently. I think the lower end of their recommendation, 1 set of each exercise to failure twice a week, is more than sufficient to meet the goal of maximizing improvements in body composition in most people. My current routine is one brief strength training session and one sprint session per week (in addition to my leisurely cycle commute), which works well for me on a cost-benefit level. However, I was stronger when I was strength training twice a week and never going to muscular failure (a la Pavel Tsatsouline).
Chapter 5, "Environment", is an interesting discussion of different factors that promote excessive calorie intake, such as the setting of the meal, the company or lack thereof, and food presentation. While they support their statements very well with evidence from scientific studies, I do have a lingering doubt about these types of studies: as far as I know, they're all based on short-term interventions. Science would be a lot easier if short-term always translated to long term, but unfortunately that's not the case. For example, studies lasting one or two weeks show that low glycemic index foods cause a reduction in calorie intake and greater feelings of fullness. However, this effect disappears in the long term, and numerous controlled trials show that low glycemic index diets have no effect on food intake, body weight or insulin sensitivity in the long term. I reviewed those studies here.
The body has homeostatic mechanisms (homeostatic = maintains the status quo) that regulate long-term energy balance. Whether short-term changes in calorie intake based on environmental cues would translate into sustained changes that would have a significant impact on body fat, I don't know. For example, if you eat a meal with your extended family at a restaurant that serves massive portions, you might eat twice as much as you would by yourself in your own home. But the question is, will your body factor that huge meal into your subsequent calorie intake and energy expenditure over the following days? The answer is clearly yes, but the degree of compensation is unclear. Since I'm not aware of any trials indicating that changing meal context can actually lead to long-term weight loss, I can't put much faith in this strategy (if you know otherwise, please link to the study in the comments).
Chapter 6, "Diet", is a very brief discussion of what to eat for weight loss. They basically recommend a low-calorie, low-carb diet focused on whole, natural foods. I think low-carbohydrate diets can be useful for some overweight people trying to lose weight, if for no other reason than the fact that they make it easier to control appetite. In addition, a subset of people respond very well to carbohydrate restriction in terms of body composition, health and well-being. The authors emphasize nutrient density, but don't really explain how to achieve it. It would have been nice to see a discussion of a few topics such as organ meats, leafy greens, dairy quality (pastured vs. conventional) and vitamin D. These may not help you lose weight, but they will help keep you healthy, particularly on a calorie-restricted diet. The authors also recommend a few energy bars, powders and supplements that I don't support. They state that they have no financial connection to the manufacturers of the products they recommend.
I'm wary of their recommendation to deliberately restrict calorie intake. Although it will clearly cause fat loss if you restrict calories enough, it's been shown to be ineffective for sustainable, long-term fat loss over and over again. The only exception is the rare person with an iron will who is able to withstand misery indefinitely. I'm going to keep an open mind on this question though. There may be a place for deliberate calorie restriction in the right context. But at this point I'm going to require some pretty solid evidence that it's effective, sustainable, and doesn't have unacceptable side effects.
The book contains a nice bonus, an appendix titled "What is Quality Evidence"? It's a brief discussion of common logical pitfalls when evaluating evidence, and I think many people could benefit from reading it.
Overall, S.P.E.E.D. was a worthwhile read, definitely superior to 95% of fat loss books. With some caveats mentioned above, I think it could be a useful resource for someone interested in fat loss.
Thursday, February 25, 2010
Corn Oil and Cancer: Reality Strikes Again
The benefits of corn oil keep rolling in. In a new study by Stephen Freedland's group at Duke, feeding mice a diet rich in butter and lard didn't promote the growth of transplanted human prostate cancer cells any more than a low-fat diet (1).
Why do we care? Because other studies, including one from the same investigators, show that corn oil and other industrial seed oils strongly promote prostate cancer cell growth and increase mortality in similar models (2, 3).
From the discussion section:
I do have one gripe with the study. They refer to the diet as "saturated fat based". That's inaccurate terminology. I see it constantly in the diet-health literature. If it were coconut oil, then maybe I could excuse it, because coconut fat is 93% saturated. But this diet was made of lard and butter, the combination of which is probably about half saturated. The term "animal fat" or "low-omega-6 fat" would have been more accurate. At least they listed the diet composition. Many studies don't even bother, leaving it to the reader to decide what they mean by "saturated fat".
* The average American eats 7-8% omega-6 by calories. This means it will be difficult to see a relationship between omega-6 intake and cancer (or heart disease, or most things) in observational studies in the US or other industrial nations, because we virtually all eat more than 4% of calories as omega-6. Until the 20th century, omega-6 intake was below 4%, and usually closer to 2%, in most traditional societies. That's where it remains in contemporary traditional societies unaffected by industrial food habits, such as Kitava. Our current omega-6 intake is outside the evolutionary norm.
Why do we care? Because other studies, including one from the same investigators, show that corn oil and other industrial seed oils strongly promote prostate cancer cell growth and increase mortality in similar models (2, 3).
From the discussion section:
Current results combined with our prior results suggest that lowering the fat content of a primarily saturated fat diet offers little survival benefit in an intact or castrated LAPC-4 xenograft model. In contrast to the findings when omega-6 fats are used, these results raise the possibility that fat type may be as important as fat amount or perhaps even more important.The authors seem somewhat surprised and pained by the result. Kudos for publishing it. However, there's nothing to be surprised about. There's a large body of evidence implicating excess omega-6 fat in a number of cancer models. Reducing omega-6 to below 4% of calories has a dramatic effect on cancer incidence and progression*. In fact, there have even been several experiments showing that butter and other animal fats promote cancer growth to a lesser degree than margarine and omega-6-rich seed oils. I discussed that here.
I do have one gripe with the study. They refer to the diet as "saturated fat based". That's inaccurate terminology. I see it constantly in the diet-health literature. If it were coconut oil, then maybe I could excuse it, because coconut fat is 93% saturated. But this diet was made of lard and butter, the combination of which is probably about half saturated. The term "animal fat" or "low-omega-6 fat" would have been more accurate. At least they listed the diet composition. Many studies don't even bother, leaving it to the reader to decide what they mean by "saturated fat".
* The average American eats 7-8% omega-6 by calories. This means it will be difficult to see a relationship between omega-6 intake and cancer (or heart disease, or most things) in observational studies in the US or other industrial nations, because we virtually all eat more than 4% of calories as omega-6. Until the 20th century, omega-6 intake was below 4%, and usually closer to 2%, in most traditional societies. That's where it remains in contemporary traditional societies unaffected by industrial food habits, such as Kitava. Our current omega-6 intake is outside the evolutionary norm.
Monday, February 22, 2010
Magnesium and Insulin Sensitivity
From a paper based on US NHANES nutrition and health survey data (1):
Magnesium status is associated with insulin sensitivity (2, 3), and a low magnesium intake predicts the development of type II diabetes in most studies (4, 5) but not all (6). Magnesium supplements largely prevent diabetes in a rat model* (7). Interestingly, excess blood glucose and insulin themselves seem to reduce magnesium status, possibly creating a vicious cycle.
In a 1993 trial, a low-magnesium diet reduced insulin sensitivity in healthy volunteers by 25% in just four weeks (8). It also increased urinary thromboxane concentration, a potential concern for cardiovascular health**.
At least three trials have shown that magnesium supplementation increases insulin sensitivity in insulin-resistant diabetics and non-diabetics (9, 10, 11). In some cases, the results were remarkable. In type II diabetics, 16 weeks of magnesium supplementation improved fasting glucose, calculated insulin sensitivity and HbA1c*** (12). HbA1c dropped by 22 percent.
In insulin resistant volunteers with low blood magnesium, magnesium supplementation for four months reduced estimated insulin resistance by 43 percent and decreased fasting insulin by 32 percent (13). This suggests to me that magnesium deficiency was probably one of the main reasons they were insulin resistant in the first place. But the study had another very interesting finding: magnesium improved the subjects' blood lipid profile remarkably. Total cholesterol decreased, LDL decreased, HDL increased and triglycerides decreased by a whopping 39 percent. The same thing had been reported in the medical literature decades earlier when doctors used magnesium injections to treat heart disease, and also in animals treated with magnesium. Magnesium supplementation also suppresses atherosclerosis (thickening and hardening of the arteries) in animal models, a fact that I may discuss in more detail at some point (14, 15).
In the previous study, participants were given 2.5 g magnesium chloride (MgCl2) per day. That's a bit more than the USDA recommended daily allowance (MgCl2 is mostly chloride by weight), in addition to what they were already getting from their diet. Most of a person's magnesium is in their bones, so correcting a deficiency by eating a nutritious diet may take a while.
Speaking of nutritious diets, how does one get magnesium? Good sources include halibut, leafy greens, chocolate and nuts. Bone broths are also an excellent source of highly absorbable magnesium. Whole grains and beans are also fairly good sources, while refined grains lack most of the magnesium in the whole grain. Organic foods, particularly artisanally produced foods from a farmer's market, are richer in magnesium because they grow on better soil and often use older varieties that are more nutritious.
The problem with seeds such as grains, beans and nuts is that they also contain phytic acid which prevents the absorption of magnesium and other minerals (16). Healthy non-industrial societies that relied on grains took great care in their preparation: they soaked them, often fermented them, and also frequently removed a portion of the bran before cooking (17). These steps all served to reduce the level of phytic acid and other anti-nutrients. I've posted a method for effectively reducing the amount of phytic acid in brown rice (18). Beans should ideally be soaked for 24 hours before cooking, preferably in warm water.
Industrial agriculture has systematically depleted our soil of many minerals, due to high-yield crop varieties and the fact that synthetic fertilizers only replace a few minerals. The mineral content of foods in the US, including magnesium, has dropped sharply in the last 50 years. The reason we need to use fertilizers in the first place is that we've broken the natural nutrient cycle in which minerals always return to the soil in the same place they were removed. In 21st century America, minerals are removed from the soil, pass through our toilets, and end up in the landfill or in waste water. This will continue until we find an acceptable way to return human feces and urine to agricultural soil, as many cultures do to this day****.
I believe that an adequate magnesium intake is critical for proper insulin sensitivity and overall health.
* Zucker rats that lack leptin signaling
** Thromboxane A2 is an omega-6 derived eicosanoid that potently constricts blood vessels and promotes blood clotting. It's interesting that magnesium has such a strong effect on it. It indicates that fatty acid balance is not the only major influence on eicosanoid production.
*** Glycated hemoglobin. A measure of the average blood glucose level over the past few weeks.
**** Anyone interested in further reading on this should look up The Humanure Handbook
During 1999–2000, the diet of a large proportion of the U.S. population did not contain adequate magnesium... Furthermore, racial or ethnic differences in magnesium persist and may contribute to some health disparities.... Because magnesium intake is low among many people in the United States and inadequate magnesium status is associated with increased risk of acute and chronic conditions, an urgent need exists to perform a current survey to assess the physiologic status of magnesium in the U.S. population.Magnesium is an essential mineral that's slowly disappearing from the modern diet, as industrial agriculture and industrial food processing increasingly dominate our food choices. One of the many things it's necessary for in mammals is proper insulin sensitivity and glucose control. A loss of glucose control due to insulin resistance can eventually lead to diabetes and all its complications.
Magnesium status is associated with insulin sensitivity (2, 3), and a low magnesium intake predicts the development of type II diabetes in most studies (4, 5) but not all (6). Magnesium supplements largely prevent diabetes in a rat model* (7). Interestingly, excess blood glucose and insulin themselves seem to reduce magnesium status, possibly creating a vicious cycle.
In a 1993 trial, a low-magnesium diet reduced insulin sensitivity in healthy volunteers by 25% in just four weeks (8). It also increased urinary thromboxane concentration, a potential concern for cardiovascular health**.
At least three trials have shown that magnesium supplementation increases insulin sensitivity in insulin-resistant diabetics and non-diabetics (9, 10, 11). In some cases, the results were remarkable. In type II diabetics, 16 weeks of magnesium supplementation improved fasting glucose, calculated insulin sensitivity and HbA1c*** (12). HbA1c dropped by 22 percent.
In insulin resistant volunteers with low blood magnesium, magnesium supplementation for four months reduced estimated insulin resistance by 43 percent and decreased fasting insulin by 32 percent (13). This suggests to me that magnesium deficiency was probably one of the main reasons they were insulin resistant in the first place. But the study had another very interesting finding: magnesium improved the subjects' blood lipid profile remarkably. Total cholesterol decreased, LDL decreased, HDL increased and triglycerides decreased by a whopping 39 percent. The same thing had been reported in the medical literature decades earlier when doctors used magnesium injections to treat heart disease, and also in animals treated with magnesium. Magnesium supplementation also suppresses atherosclerosis (thickening and hardening of the arteries) in animal models, a fact that I may discuss in more detail at some point (14, 15).
In the previous study, participants were given 2.5 g magnesium chloride (MgCl2) per day. That's a bit more than the USDA recommended daily allowance (MgCl2 is mostly chloride by weight), in addition to what they were already getting from their diet. Most of a person's magnesium is in their bones, so correcting a deficiency by eating a nutritious diet may take a while.
Speaking of nutritious diets, how does one get magnesium? Good sources include halibut, leafy greens, chocolate and nuts. Bone broths are also an excellent source of highly absorbable magnesium. Whole grains and beans are also fairly good sources, while refined grains lack most of the magnesium in the whole grain. Organic foods, particularly artisanally produced foods from a farmer's market, are richer in magnesium because they grow on better soil and often use older varieties that are more nutritious.
The problem with seeds such as grains, beans and nuts is that they also contain phytic acid which prevents the absorption of magnesium and other minerals (16). Healthy non-industrial societies that relied on grains took great care in their preparation: they soaked them, often fermented them, and also frequently removed a portion of the bran before cooking (17). These steps all served to reduce the level of phytic acid and other anti-nutrients. I've posted a method for effectively reducing the amount of phytic acid in brown rice (18). Beans should ideally be soaked for 24 hours before cooking, preferably in warm water.
Industrial agriculture has systematically depleted our soil of many minerals, due to high-yield crop varieties and the fact that synthetic fertilizers only replace a few minerals. The mineral content of foods in the US, including magnesium, has dropped sharply in the last 50 years. The reason we need to use fertilizers in the first place is that we've broken the natural nutrient cycle in which minerals always return to the soil in the same place they were removed. In 21st century America, minerals are removed from the soil, pass through our toilets, and end up in the landfill or in waste water. This will continue until we find an acceptable way to return human feces and urine to agricultural soil, as many cultures do to this day****.
I believe that an adequate magnesium intake is critical for proper insulin sensitivity and overall health.
* Zucker rats that lack leptin signaling
** Thromboxane A2 is an omega-6 derived eicosanoid that potently constricts blood vessels and promotes blood clotting. It's interesting that magnesium has such a strong effect on it. It indicates that fatty acid balance is not the only major influence on eicosanoid production.
*** Glycated hemoglobin. A measure of the average blood glucose level over the past few weeks.
**** Anyone interested in further reading on this should look up The Humanure Handbook
Lindeberg on Obesity
I'm currently reading Dr. Staffan Lindeberg's magnum opus Food and Western Disease, recently published in English for the first time. Dr. Lindeberg is one of the world's leading experts on the health and diet of non-industrial cultures, particularly in Papua New Guinea. The book contains 2,034 references. It's also full of quotable statements. Here's what he has to say about obesity:
I'd recommend this book to anyone who has a scholarly interest in health and nutrition, and somewhat of a background in science and medicine. It's extremely well referenced, which makes it much more valuable.
Middle-age spread is a normal phenomenon - assuming you live in the West. Few people are able to maintain their [youthful] waistline after age 50. The usual explanation - too little exercise and too much food - does not fully take into account the situation among traditional populations. Such people are usually not as physically active as you may think, and they usually eat large quantities of food.The only obese Kitavans Dr. Lindeberg observed were two people who had spent several years off the island living a modern, urban lifestyle, and were back on Kitava for a visit.
Overweight has been extremely rare among hunter-gatherers and other traditional cultures [18 references]. This simple fact has been quickly apparent to all foreign visitors...
The Kitava study measured height, weight, waist circumference, subcutaneous fat thickness at the back of the upper arm (triceps skinfold) and upper arm circumference on 272 persons ages 4-86 years. Overweight and obesity were absent and average [body mass index] was low across all age groups. ...no one was larger around their waist than around their hips.
...The circumference of the upper arm [mostly indicating muscle mass] was only negligibly smaller on Kitava [compared with Sweden], which indicates that there was no malnutrition. It is obvious from our investigations that lack of food is an unknown concept, and that the surplus of fruits and vegetables regularly rots or is eaten by dogs.
The Population of Kitava occupies a unique position in the world in terms of the negligible effect that the Western lifestyle has had on the island.
I'd recommend this book to anyone who has a scholarly interest in health and nutrition, and somewhat of a background in science and medicine. It's extremely well referenced, which makes it much more valuable.
Tuesday, February 16, 2010
Dissolve Away those Pesky Bones with Corn Oil
I just read an interesting paper from Gabriel Fernandes's group at the University of Texas. It's titled "High fat diet-induced animal model of age-associated obesity and osteoporosis". I was expecting this to be the usual "we fed mice industrial lard for 60% of calories and they got sick" paper, but I was pleasantly surprised. From the introduction:
20% fat is less than the amount it typically takes to make a rodent this sick. This leads me to conclude that corn oil is particularly good at causing mouse versions of some of the most common facets of the "diseases of civilization". It's exceptionally high in omega-6 (linoleic acid) with virtually no omega-3.
Make sure to eat your heart-healthy corn oil! It's made in the USA, dirt cheap and it even lowers cholesterol!
CO [corn oil] is known to promote bone loss, obesity, impaired glucose tolerance, insulin resistance and thus represents a useful model for studying the early stages in the development of obesity, hyperglycemia, Type 2 diabetes [23] and osteoporosis. We have used omega-6 fatty acids enriched diet as a fat source which is commonly observed in today's Western diets basically responsible for the pathogenesis of many diseases [24].Just 10% of the diet as corn oil (roughly 20% of calories), with no added omega-3, on top of an otherwise poor laboratory diet, caused:
- Obesity
- Osteoporosis
- The replacement of bone marrow with fat cells
- Diabetes
- Insulin resistance
- Generalized inflammation
- Elevated liver weight (possibly indicating fatty liver)
20% fat is less than the amount it typically takes to make a rodent this sick. This leads me to conclude that corn oil is particularly good at causing mouse versions of some of the most common facets of the "diseases of civilization". It's exceptionally high in omega-6 (linoleic acid) with virtually no omega-3.
Make sure to eat your heart-healthy corn oil! It's made in the USA, dirt cheap and it even lowers cholesterol!
Tuesday, February 9, 2010
Saturated Fat and Insulin Sensitivity
Insulin sensitivity is a measure of the tissue response to insulin. Typically, it refers to insulin's ability to cause tissues to absorb glucose from the blood. A loss of insulin sensitivity, also called insulin resistance, is a core part of the metabolic disorder that affects many people in industrial nations.
I don't know how many times I've seen the claim in journal articles and on the internet that saturated fat reduces insulin sensitivity. The idea is that saturated fat reduces the body's ability to handle glucose effectively, placing people on the road to diabetes, obesity and heart disease. Given the "selective citation disorder" that plagues the diet-health literature, perhaps this particular claim deserves a closer look.
The Evidence
I found a review article from 2008 that addressed this question (1). I like this review because it only includes high-quality trials that used reliable methods of determining insulin sensitivity*.
On to the meat of it. There were 5 studies in which non-diabetic people were fed diets rich in saturated fat, and compared with a group eating a diet rich in monounsaturated (like olive oil) or polyunsaturated (like corn oil) fat. They ranged in duration from one week to 3 months. Four of the five studies found that fat quality did not affect insulin sensitivity, including one of the 3-month studies.
The fifth study, which is the one that's nearly always cited in the diet-health literature, requires some discussion. This was the KANWU study (2). Over the course of three months, investigators fed 163 volunteers a diet rich in either saturated fat or monounsaturated fat.
What the authors decided to focus on instead is the fact that insulin sensitivity declined slightly but significantly on the saturated fat diet compared with the pre-diet baseline. That's why this study is cited as evidence that saturated fat impairs insulin sensitivity. But anyone who has a basic science background will see where this reasoning is flawed (warning: nerd attack. skip the rest of the paragraph if you're not interested). You need a control group for comparison, to take into account normal fluctuations caused by such things as the season, eating mostly cafeteria food, and having a doctor hooking you up to machines. That control group was the group eating monounsaturated fat. The comparison between diet groups was the 'primary outcome', in statistics lingo. That's the comparison that matters, and it wasn't significant. To interpret the study otherwise is to ignore the basic conventions of statistics, which the authors were happy to do. There's a name for it: 'moving the goalpost'. The reviewers shouldn't have let this kind of shenanigans slide.
So we have five studies through 2008, none of which support the idea that saturated fat reduces insulin sensitivity in non-diabetics. Since the review paper was published, I know of one subsequent study that asked the same question (3). Susan J. van Dijk and colleagues fed volunteers with abdominal overweight (beer gut) a diet rich in either saturated fat or monounsaturated fat. I e-mailed the senior author and she said the saturated fat diet was "mostly butter". The specific fats used in the diets weren't mentioned anywhere in the paper, which is a major omission**. In any case, after 8 weeks, insulin sensitivity was virtually identical between the two groups. This study appeared well controlled and used the gold standard method for assessing insulin sensitivity, called the euglycemic-hyperinsulinemic clamp technique***.
The evidence from controlled trials is rather consistent that saturated fat has no appreciable effect on insulin sensitivity.
Why Are We so Focused on Saturated Fat?
Answer: because it's the nutrient everyone loves to hate. As an exercise in completeness, I'm going to mention three dietary factors that actually reduce insulin sensitivity, and get a lot less air time than saturated fat.
#1: Caffeine. That's right, controlled trials show that your favorite murky beverage reduces insulin sensitivity (4, 5). Is it actually relevant to real life? I doubt it. The doses used were large and the studies short-term.
#2: Magnesium deficiency. A low-magnesium diet reduced insulin sensitivity by 25% over the course of three weeks (6). I think this is probably relevant to long-term insulin sensitivity and overall health, although it would be good to have longer-term data. Magnesium deficiency is widespread in industrial nations, due to our over-reliance on refined foods such as sugar, white flour and oils.
#3: Sugar. Fructose reduces insulin sensitivity in humans, along with many other harmful effects (7).
As long as we continue to focus our energy on indicting saturated fat, it will continue distracting us from the real causes of disease.
* For the nerds: euglycemic-hyperinsulinemic clamp (the gold standard), insulin suppression test, or intravenous glucose tolerance test with Minimal Model. They didn't include studies that reported HOMA as their only measure, because it's not very accurate.
** There's this idea that pervades the diet-health literature that all saturated fats are roughly equivalent, all monounsaturated fats are equivalent, etc., therefore it doesn't matter what the source was. This is beyond absurd and reflects our cultural obsession with saturated fat. It really irks me that the reviewers didn't demand this information.
*** They did find that markers of inflammation in fat tissue were higher after the saturated fat diet.
I don't know how many times I've seen the claim in journal articles and on the internet that saturated fat reduces insulin sensitivity. The idea is that saturated fat reduces the body's ability to handle glucose effectively, placing people on the road to diabetes, obesity and heart disease. Given the "selective citation disorder" that plagues the diet-health literature, perhaps this particular claim deserves a closer look.
The Evidence
I found a review article from 2008 that addressed this question (1). I like this review because it only includes high-quality trials that used reliable methods of determining insulin sensitivity*.
On to the meat of it. There were 5 studies in which non-diabetic people were fed diets rich in saturated fat, and compared with a group eating a diet rich in monounsaturated (like olive oil) or polyunsaturated (like corn oil) fat. They ranged in duration from one week to 3 months. Four of the five studies found that fat quality did not affect insulin sensitivity, including one of the 3-month studies.
The fifth study, which is the one that's nearly always cited in the diet-health literature, requires some discussion. This was the KANWU study (2). Over the course of three months, investigators fed 163 volunteers a diet rich in either saturated fat or monounsaturated fat.
The SAFA diet included butter and a table margarine containing a relatively high proportion of SAFAs. The MUFA diet included a spread and a margarine containing high proportions of oleic acid derived from high-oleic sunflower oil and negligible amounts of trans fatty acids and n-3 fatty acids and olive oil.Yummy. After three months of these diets, there was no significant difference in insulin sensitivity between the saturated fat group and the monounsaturated fat group. Yes, you read that right. Even the study that's selectively cited as evidence that saturated fat causes insulin resistance found no significant difference between the diets. You might not get this by reading the misleading abstract. I'll be generous and acknowledge that the (small) difference was almost statistically significant (p = 0.053).
What the authors decided to focus on instead is the fact that insulin sensitivity declined slightly but significantly on the saturated fat diet compared with the pre-diet baseline. That's why this study is cited as evidence that saturated fat impairs insulin sensitivity. But anyone who has a basic science background will see where this reasoning is flawed (warning: nerd attack. skip the rest of the paragraph if you're not interested). You need a control group for comparison, to take into account normal fluctuations caused by such things as the season, eating mostly cafeteria food, and having a doctor hooking you up to machines. That control group was the group eating monounsaturated fat. The comparison between diet groups was the 'primary outcome', in statistics lingo. That's the comparison that matters, and it wasn't significant. To interpret the study otherwise is to ignore the basic conventions of statistics, which the authors were happy to do. There's a name for it: 'moving the goalpost'. The reviewers shouldn't have let this kind of shenanigans slide.
So we have five studies through 2008, none of which support the idea that saturated fat reduces insulin sensitivity in non-diabetics. Since the review paper was published, I know of one subsequent study that asked the same question (3). Susan J. van Dijk and colleagues fed volunteers with abdominal overweight (beer gut) a diet rich in either saturated fat or monounsaturated fat. I e-mailed the senior author and she said the saturated fat diet was "mostly butter". The specific fats used in the diets weren't mentioned anywhere in the paper, which is a major omission**. In any case, after 8 weeks, insulin sensitivity was virtually identical between the two groups. This study appeared well controlled and used the gold standard method for assessing insulin sensitivity, called the euglycemic-hyperinsulinemic clamp technique***.
The evidence from controlled trials is rather consistent that saturated fat has no appreciable effect on insulin sensitivity.
Why Are We so Focused on Saturated Fat?
Answer: because it's the nutrient everyone loves to hate. As an exercise in completeness, I'm going to mention three dietary factors that actually reduce insulin sensitivity, and get a lot less air time than saturated fat.
#1: Caffeine. That's right, controlled trials show that your favorite murky beverage reduces insulin sensitivity (4, 5). Is it actually relevant to real life? I doubt it. The doses used were large and the studies short-term.
#2: Magnesium deficiency. A low-magnesium diet reduced insulin sensitivity by 25% over the course of three weeks (6). I think this is probably relevant to long-term insulin sensitivity and overall health, although it would be good to have longer-term data. Magnesium deficiency is widespread in industrial nations, due to our over-reliance on refined foods such as sugar, white flour and oils.
#3: Sugar. Fructose reduces insulin sensitivity in humans, along with many other harmful effects (7).
As long as we continue to focus our energy on indicting saturated fat, it will continue distracting us from the real causes of disease.
* For the nerds: euglycemic-hyperinsulinemic clamp (the gold standard), insulin suppression test, or intravenous glucose tolerance test with Minimal Model. They didn't include studies that reported HOMA as their only measure, because it's not very accurate.
** There's this idea that pervades the diet-health literature that all saturated fats are roughly equivalent, all monounsaturated fats are equivalent, etc., therefore it doesn't matter what the source was. This is beyond absurd and reflects our cultural obsession with saturated fat. It really irks me that the reviewers didn't demand this information.
*** They did find that markers of inflammation in fat tissue were higher after the saturated fat diet.
Sunday, February 7, 2010
Thank You
I'd like to extend my sincere thanks to everyone who has supported me through donations this year. The money has allowed me to buy materials that I wouldn't otherwise have been able to afford, and I feel it has enriched the blog for everyone. Here are some of the books I've bought using donations. Some were quite expensive:
Food and western disease: health and nutrition from an evolutionary perspective. Staffan Lindeberg (just released!!)
Nutrition and disease. Edward Mellanby
Migration and health in a small society: the case of Tokelau. Edited by Albert F. Wessen
The saccharine disease. T. L. Cleave
Culture, ecology and dental anthropology. John R. Lukacs
Vitamin K in health and disease. John W. Suttie
Craniofacial development. Geoffrey H. Sperber
Western diseases: their emergence and prevention. Hugh C. Trowell and Denis P. Burkitt
The ultimate omega-3 diet. Evelyn Tribole
Our changing fare. John Yudkin and colleagues
Donations have also paid for many, many photocopies at the medical library. I'd also like to thank everyone who participates in the community by leaving comments, or by linking to my posts. I appreciate your encouragement, and also the learning opportunities.
Food and western disease: health and nutrition from an evolutionary perspective. Staffan Lindeberg (just released!!)
Nutrition and disease. Edward Mellanby
Migration and health in a small society: the case of Tokelau. Edited by Albert F. Wessen
The saccharine disease. T. L. Cleave
Culture, ecology and dental anthropology. John R. Lukacs
Vitamin K in health and disease. John W. Suttie
Craniofacial development. Geoffrey H. Sperber
Western diseases: their emergence and prevention. Hugh C. Trowell and Denis P. Burkitt
The ultimate omega-3 diet. Evelyn Tribole
Our changing fare. John Yudkin and colleagues
Donations have also paid for many, many photocopies at the medical library. I'd also like to thank everyone who participates in the community by leaving comments, or by linking to my posts. I appreciate your encouragement, and also the learning opportunities.
Sunday, January 31, 2010
The Body Fat Setpoint, Part IV: Changing the Setpoint
Prevention is Easier than Cure
Experiments in animals have confirmed what common sense suggests: it's easier to prevent health problems than to reverse them. Still, many health conditions can be improved, and in some cases reversed, through lifestyle interventions. It's important to have realistic expectations and to be kind to oneself. Cultivating a drill sergeant mentality will not improve quality of life, and isn't likely to be sustainable.
Fat Loss: a New Approach
If there's one thing that's consistent in the medical literature, it's that telling people to eat fewer calories does not help them lose weight in the long term. Gary Taubes has written about this at length in his book Good Calories, Bad Calories, and in his upcoming book on body fat. Many people who use this strategy see transient fat loss, followed by fat regain and a feeling of defeat. There's a simple reason for it: the body doesn't want to lose weight. It's extremely difficult to fight the fat mass setpoint, and the body will use every tool it has to maintain its preferred level of fat: hunger, reduced body temperature, higher muscle efficiency (i.e., less energy is expended for the same movement), lethargy, lowered immune function, et cetera.
Therefore, what we need for sustainable fat loss is not starvation; we need a treatment that lowers the fat mass setpoint. There are several criteria that this treatment will have to meet to qualify:
Strategies: Diet Pattern
The most obvious treatment that fits all of my criteria is low-carbohydrate dieting. Overweight people eating low-carbohydrate diets generally lose fat and spontaneously reduce their calorie intake. In fact, in several diet studies, investigators compared an all-you-can-eat low-carbohydrate diet with a calorie-restricted low-fat diet. The low-carbohydrate dieters generally reduced their calorie intake and body fat to a similar or greater degree than the low-fat dieters, despite the fact that they ate all the calories they wanted (1). This suggest that their fat mass setpoint had changed. At this point, I think moderate carbohydrate restriction may be preferable to strict carbohydrate restriction for some people, due to the increasing number of reports I've read of people doing poorly in the long run on extremely low-carbohydrate diets (2).
Another strategy that appears effective is the "paleolithic" diet. In Dr. Staffan Lindeberg's 2007 diet study, overweight volunteers with heart disease lost fat and reduced their calorie intake to a remarkable degree while eating a diet consistent with our hunter-gatherer heritage (3). This result is consistent with another diet trial of the paleolithic diet in diabetics (4). In post hoc analysis, Dr. Lindeberg's group showed that the reduction in weight was apparently independent of changes in carbohydrate intake*. This suggests that the paleolithic diet has health benefits that are independent of carbohydrate intake.
Strategies: Gastrointestinal Health
Since the gastrointestinal (GI) tract is so intimately involved in body fat metabolism and overall health (see the former post), the next strategy is to improve GI health. There are a number of ways to do this, but they all center around four things:
Oligofructose is similar to inulin, a fiber that occurs naturally in a wide variety of plants. Good sources are jerusalem artichokes, jicama, artichokes, onions, leeks, burdock and chicory root. Certain non-industrial cultures had a high intake of inulin. There are some caveats to inulin, however: inulin and oligofructose can cause gas, and can also exacerbate gastroesophageal reflux disorder (9). So don't eat a big plate of jerusalem artichokes before that important date.
The colon is packed with symbiotic bacteria, and is the site of most intestinal fermentation. The small intestine contains fewer bacteria, but gut barrier function there is critical as well. The small intestine is where the GI doctor will take a biopsy to look for celiac disease. Celiac disease is a degeneration of the small intestinal lining due to an autoimmune reaction caused by gluten (in wheat, barley and rye). This brings us to one of the most important elements of maintaining gut barrier health: avoiding food sensitivities. Gluten and casein (in dairy protein) are the two most common offenders. Gluten sensitivity is widespread and typically undiagnosed (10).
Eating raw fermented foods such as sauerkraut, kimchi, yogurt and half-sour pickles also helps maintain the integrity of the upper GI tract. I doubt these have any effect on the colon, given the huge number of bacteria already present. Other important factors in gut barrier health are keeping the ratio of omega-6 to omega-3 fats in balance, eating nutrient-dense food, and avoiding the questionable chemical additives in processed food. If triglycerides are important for leptin sensitivity, then avoiding sugar and ensuring a regular source of omega-3 should aid weight loss as well.
Strategies: Micronutrients
As I discussed in the last post, micronutrient deficiency probably plays a role in obesity, both in ways that we understand and ways that we (or I) don't. Eating a diet that has a high nutrient density and ensuring a good vitamin D status will help any sustainable fat loss strategy. The easiest way to do this is to eliminate industrially processed foods such as white flour, sugar and seed oils. These constitute more than 50% of calories for the average Westerner.
After that, you can further increase your diet's nutrient density by learning to properly prepare grains and legumes to maximize their nutritional value and digestibility (11, 12; or by avoiding grains and legumes altogether if you wish), selecting organic and/or pasture-raised foods if possible, and eating seafood including seaweed. One of the problems with extremely low-carbohydrate diets is that they may be low in water-soluble micronutrients, although this isn't necessarily the case.
Strategies: Miscellaneous
In general, exercise isn't necessarily helpful for fat loss. However, there is one type of exercise that clearly is: high-intensity intermittent training (HIIT). It's basically a fancy name for sprints. They can be done on a track, on a stationary bicycle, using weight training circuits, or any other way that allows sufficient intensity. The key is to achieve maximal exertion for several brief periods, separated by rest. This type of exercise is not about burning calories through exertion: it's about increasing hormone sensitivity using an intense, brief stressor (hormesis). Even a ridiculously short period of time spent training HIIT each week can result in significant fat loss, despite no change in diet or calorie intake (13).
Anecdotally, many people have had success using intermittent fasting (IF) for fat loss. There's some evidence in the scientific literature that IF and related approaches may be helpful (14). There are different approaches to IF, but a common and effective method is to do two complete 24-hour fasts per week. It's important to note that IF isn't about restricting calories, it's about resetting the fat mass setpoint. After a fast, allow yourself to eat quality food until you're no longer hungry.
Insufficient sleep has been strongly and repeatedly linked to obesity. Whether it's a cause or consequence of obesity I can't say for sure, but in any case it's important for health to sleep until you feel rested. If your sleep quality is poor due to psychological stress, meditating before bedtime may help. I find that meditation has a remarkable effect on my sleep quality. Due to the poor development of oral and nasal structures in industrial nations, many people do not breathe effectively and may suffer from conditions such as sleep apnea that reduce sleep quality. Overweight also contributes to these problems.
I'm sure there are other useful strategies, but that's all I have for now. If you have something to add, please put it in the comments.
* Since reducing carbohydrate intake wasn't part of the intervention, this result is observational.
Experiments in animals have confirmed what common sense suggests: it's easier to prevent health problems than to reverse them. Still, many health conditions can be improved, and in some cases reversed, through lifestyle interventions. It's important to have realistic expectations and to be kind to oneself. Cultivating a drill sergeant mentality will not improve quality of life, and isn't likely to be sustainable.
Fat Loss: a New Approach
If there's one thing that's consistent in the medical literature, it's that telling people to eat fewer calories does not help them lose weight in the long term. Gary Taubes has written about this at length in his book Good Calories, Bad Calories, and in his upcoming book on body fat. Many people who use this strategy see transient fat loss, followed by fat regain and a feeling of defeat. There's a simple reason for it: the body doesn't want to lose weight. It's extremely difficult to fight the fat mass setpoint, and the body will use every tool it has to maintain its preferred level of fat: hunger, reduced body temperature, higher muscle efficiency (i.e., less energy is expended for the same movement), lethargy, lowered immune function, et cetera.
Therefore, what we need for sustainable fat loss is not starvation; we need a treatment that lowers the fat mass setpoint. There are several criteria that this treatment will have to meet to qualify:
- It must cause fat loss
- It must not involve deliberate calorie restriction
- It must maintain fat loss over a long period of time
- It must not be harmful to overall health
Strategies: Diet Pattern
The most obvious treatment that fits all of my criteria is low-carbohydrate dieting. Overweight people eating low-carbohydrate diets generally lose fat and spontaneously reduce their calorie intake. In fact, in several diet studies, investigators compared an all-you-can-eat low-carbohydrate diet with a calorie-restricted low-fat diet. The low-carbohydrate dieters generally reduced their calorie intake and body fat to a similar or greater degree than the low-fat dieters, despite the fact that they ate all the calories they wanted (1). This suggest that their fat mass setpoint had changed. At this point, I think moderate carbohydrate restriction may be preferable to strict carbohydrate restriction for some people, due to the increasing number of reports I've read of people doing poorly in the long run on extremely low-carbohydrate diets (2).
Another strategy that appears effective is the "paleolithic" diet. In Dr. Staffan Lindeberg's 2007 diet study, overweight volunteers with heart disease lost fat and reduced their calorie intake to a remarkable degree while eating a diet consistent with our hunter-gatherer heritage (3). This result is consistent with another diet trial of the paleolithic diet in diabetics (4). In post hoc analysis, Dr. Lindeberg's group showed that the reduction in weight was apparently independent of changes in carbohydrate intake*. This suggests that the paleolithic diet has health benefits that are independent of carbohydrate intake.
Strategies: Gastrointestinal Health
Since the gastrointestinal (GI) tract is so intimately involved in body fat metabolism and overall health (see the former post), the next strategy is to improve GI health. There are a number of ways to do this, but they all center around four things:
- Don't eat food that encourages the growth of harmful bacteria
- Eat food that encourages the growth of good bacteria
- Don't eat food that impairs gut barrier function
- Eat food that promotes gut barrier health
Oligofructose is similar to inulin, a fiber that occurs naturally in a wide variety of plants. Good sources are jerusalem artichokes, jicama, artichokes, onions, leeks, burdock and chicory root. Certain non-industrial cultures had a high intake of inulin. There are some caveats to inulin, however: inulin and oligofructose can cause gas, and can also exacerbate gastroesophageal reflux disorder (9). So don't eat a big plate of jerusalem artichokes before that important date.
The colon is packed with symbiotic bacteria, and is the site of most intestinal fermentation. The small intestine contains fewer bacteria, but gut barrier function there is critical as well. The small intestine is where the GI doctor will take a biopsy to look for celiac disease. Celiac disease is a degeneration of the small intestinal lining due to an autoimmune reaction caused by gluten (in wheat, barley and rye). This brings us to one of the most important elements of maintaining gut barrier health: avoiding food sensitivities. Gluten and casein (in dairy protein) are the two most common offenders. Gluten sensitivity is widespread and typically undiagnosed (10).
Eating raw fermented foods such as sauerkraut, kimchi, yogurt and half-sour pickles also helps maintain the integrity of the upper GI tract. I doubt these have any effect on the colon, given the huge number of bacteria already present. Other important factors in gut barrier health are keeping the ratio of omega-6 to omega-3 fats in balance, eating nutrient-dense food, and avoiding the questionable chemical additives in processed food. If triglycerides are important for leptin sensitivity, then avoiding sugar and ensuring a regular source of omega-3 should aid weight loss as well.
Strategies: Micronutrients
As I discussed in the last post, micronutrient deficiency probably plays a role in obesity, both in ways that we understand and ways that we (or I) don't. Eating a diet that has a high nutrient density and ensuring a good vitamin D status will help any sustainable fat loss strategy. The easiest way to do this is to eliminate industrially processed foods such as white flour, sugar and seed oils. These constitute more than 50% of calories for the average Westerner.
After that, you can further increase your diet's nutrient density by learning to properly prepare grains and legumes to maximize their nutritional value and digestibility (11, 12; or by avoiding grains and legumes altogether if you wish), selecting organic and/or pasture-raised foods if possible, and eating seafood including seaweed. One of the problems with extremely low-carbohydrate diets is that they may be low in water-soluble micronutrients, although this isn't necessarily the case.
Strategies: Miscellaneous
In general, exercise isn't necessarily helpful for fat loss. However, there is one type of exercise that clearly is: high-intensity intermittent training (HIIT). It's basically a fancy name for sprints. They can be done on a track, on a stationary bicycle, using weight training circuits, or any other way that allows sufficient intensity. The key is to achieve maximal exertion for several brief periods, separated by rest. This type of exercise is not about burning calories through exertion: it's about increasing hormone sensitivity using an intense, brief stressor (hormesis). Even a ridiculously short period of time spent training HIIT each week can result in significant fat loss, despite no change in diet or calorie intake (13).
Anecdotally, many people have had success using intermittent fasting (IF) for fat loss. There's some evidence in the scientific literature that IF and related approaches may be helpful (14). There are different approaches to IF, but a common and effective method is to do two complete 24-hour fasts per week. It's important to note that IF isn't about restricting calories, it's about resetting the fat mass setpoint. After a fast, allow yourself to eat quality food until you're no longer hungry.
Insufficient sleep has been strongly and repeatedly linked to obesity. Whether it's a cause or consequence of obesity I can't say for sure, but in any case it's important for health to sleep until you feel rested. If your sleep quality is poor due to psychological stress, meditating before bedtime may help. I find that meditation has a remarkable effect on my sleep quality. Due to the poor development of oral and nasal structures in industrial nations, many people do not breathe effectively and may suffer from conditions such as sleep apnea that reduce sleep quality. Overweight also contributes to these problems.
I'm sure there are other useful strategies, but that's all I have for now. If you have something to add, please put it in the comments.
* Since reducing carbohydrate intake wasn't part of the intervention, this result is observational.
Subscribe to:
Posts (Atom)